
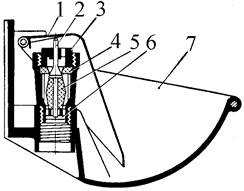
Индивидуальные и групповые автопоилки: для животных. Схемы и конструкции...
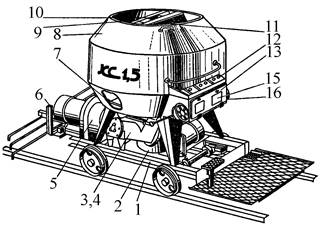
Кормораздатчик мобильный электрифицированный: схема и процесс работы устройства...
Индивидуальные и групповые автопоилки: для животных. Схемы и конструкции...
Кормораздатчик мобильный электрифицированный: схема и процесс работы устройства...
Топ:
Оснащения врачебно-сестринской бригады.
Особенности труда и отдыха в условиях низких температур: К работам при низких температурах на открытом воздухе и в не отапливаемых помещениях допускаются лица не моложе 18 лет, прошедшие...
Выпускная квалификационная работа: Основная часть ВКР, как правило, состоит из двух-трех глав, каждая из которых, в свою очередь...
Интересное:
Распространение рака на другие отдаленные от желудка органы: Характерных симптомов рака желудка не существует. Выраженные симптомы появляются, когда опухоль...
Подходы к решению темы фильма: Существует три основных типа исторического фильма, имеющих между собой много общего...
Влияние предпринимательской среды на эффективное функционирование предприятия: Предпринимательская среда – это совокупность внешних и внутренних факторов, оказывающих влияние на функционирование фирмы...
Дисциплины:
|
из
5.00
|
Заказать работу |
|
|
|
|
Definition of Erectile Dysfunction
Erectile dysfunction (ED) is defined as the persistent inability to achieve or maintain penile erection sufficient for satisfactory sexual performance.1 The 1992 National Institutes of Health (NIH) Consensus Development Conference recommended the use of erectile dysfunction as the preferred term to impotence, the former being more precise.1 There is no universal consensus or agreed criteria as to how consistent the problem (i.e., inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance) has to be and for what duration it should last to fulfill this definition. A period of persistence over 3 months has been suggested as a reasonable clinical guideline.1, 2
Physiology of Erection
Penile erection is a complex process involving interactions between neural, psychological, vascular, and hormonal factors. The pathway of normal sexual function in males consists of four stages: sexual desire (i.e., libido), erection, ejaculation (i.e., orgasm), and detumescence (penile flaccidity).3 The erection cycle is initiated by sexual stimulation. Erection subsides at ejaculation or cessation of sexual stimulation and the subsequent flaccidity state is maintained until the next sexual stimulation or nocturnal erection occurs. Thus, both the erection and the flaccidity states of the penis exist in two phases, initiation and maintenance. Pathways responsible for penile flaccidity are no less important than pro-erectile mechanisms, and may play critical roles in certain types of erectile dysfunction (ED).4 Additionally, hormones function not only at the libido level, but help maintain anatomical and physiological integrity of penile cavernosal structures; testosterone deficiency interferes not only with normal function, but can also diminish response to ED treatment.5
The mechanism of erection involves responses to external sensory stimuli through parasympathetic activity, which leads to release of nitric oxide (NO) from nonadrenergic-noncholinergic (NANC) cavernous (penile) nerve endings and the endothelium of the penis. The initial phase of smooth muscle relaxation results in reduced peripheral resistance of cavernosal arterioles and thereby allows blood to flow into the penis under the driving force of systemic blood pressure.4 Once blood rushes into the sinusoids of the corpora cavernosa, shear stress can also release NO from endothelium to augment smooth muscle relaxation and erection. In addition, oxygen tension and substances secreted by endothelium lining the sinusoidal spaces, (i.e. prostaglandins, endothelins, and angiotensin) may also be involved in penile erection and detumescence.6, 7
The somatic sensory nerves originate at receptors in the penis to transmit pain, temperature, touch, and vibratory sensations, and the brain modulates the spinal pathways of erection via the medial preoptic area and paraventricular nucleus of the hypothalamus, periaqueductal gray of the midbrain, and the nucleus paragigantocellularis of the medulla.3 During sexual stimulation, NO released from the penile cavernosal nerve endings and endothelium, diffuses into the trabecular and arterial smooth muscle cells to activate guanylyl cyclase, thereby catalyzing the formation of second messenger cyclic guanosine monophasphate (cGMP). The cGMP in turn activates protein kinase G, phosphorylating potassium and calcium channels; the end result is hyperpolarization, reduced intracytosolic calcium, and dissociation of the myosin head from acting as smooth muscle relaxes. Cyclic adenosinemonophosphate (cAMP) is another second messenger involved in smooth muscle relaxation and is activated by cAMP-signaling molecules including adenosine, calcitonin gene-related peptides, and prostaglandins.4
|
|
On the other hand, norepinephrine, phenylephrine, and endothelin appear to activate phospholipase C, leading to the formation of inositol triphosphate and diacylglycerol. The net result is increased cytoplasmic calcium and subsequent smooth-muscle contraction. Detumescence occurs following degradation of cGMP and cAMP to GMP and AMP, respectively, by specific phosphodiesterases. Sympathetic discharge occurs if sexual stimulation results in ejaculation.8, 9 Activated Rho-kinase phosphorylates, inhibits the regulatory subunit of smooth muscle myosin phosphatase, preventing dephosphorylation of myofilaments and maintaining contractile tone.10 In the flaccid state, these smooth muscles are tonically contracted due to intrinsic smooth-muscle tone, adrenergic discharge, and other signaling molecules such as endothelin.4
Определение эректильной дисфункции
Эректильная дисфункция (ЭД) определяется как устойчивая неспособность достигать или поддерживать эрекцию полового члена, достаточную для проведения коитуса.1 В 1992 Национальный институт здоровья (NIH) на конференции по развитию рекомендовал использовать термин «эректильной дисфункции» в качестве более предпочтительного вместо импотенции.1 На тот момент не существовало согласованных критериев относительно того, как сформировать проблему (т.е. неспособность достигать или поддерживать эрекцию полового члена, достаточную для успешного полового акта) и как долго должна наблюдаться дисфункция чтобы соответствовать данному определению. Период в течение 3 месяцев был предложен в качестве наиболее разумного.1, 2
Физиология эрекции
Эрекция полового члена представляет собой сложный процесс, включающий взаимодействие между нервной системой, сосудистой системой, гормональных факторов и психологических аспектов. Нормальная сексуальная функция мужчины состоит из четырех этапов: сексуального желания (т.е. либидо), эрекции, эякуляции (т.е., оргазма), и детумесценции.3 Данный цикл инициируется сексуальной стимуляцией. Эрекция прекращается после эякуляции или прекращения сексуальной стимуляции с последующим поддерживающимся состоянием детумесценции, пока не произойдет следующая сексуальная стимуляция или ночная эрекция. Таким образом, и состояния эрекции и состояние вялости полового члена осуществляются в два этапа: инициирования и поддержания. Не Пути, ответственные за полового члена вялости не менее важны, чем про- эректильной механизмов, и может играть решающую роль в некоторых видах эректильной дисфункции (ЭД) 0,4 Кроме того, гормоны функционировать не только на уровне либидо, но поможет сохранить анатомическую и физиологическую целостность полового члена кавернозных структур; дефицит тестостерона препятствует не только с нормальной функцией, но также может уменьшить ответ на ED treatment.5
|
|
Механизм эрекции предполагает ответов на внешних сенсорных стимулов через парасимпатической активности, что приводит к высвобождению оксида азота (NO) из неадренергических - нехолинергических (NANC) кавернозных (полового члена) нервных окончаний и эндотелия пениса. Начальная фаза гладких результатов расслабления мышц в сниженной периферической сопротивления кавернозных артериол и тем самым позволяет крови течь в пенис под движущей силой системного pressure.4 крови После кровь приливает в синусоиды кавернозных тел, напряжение сдвига может также освободить НЕТ от эндотелия, чтобы увеличить расслабление гладкой мышцы и эрекцию. Кроме того, напряжения кислорода и веществ, выделяемых эндотелия, выстилающих синусоиды пространства, (т.е. простагландины, Эндотелины и ангиотензина) также могут быть вовлечены в эрекции полового члена и detumescence.6, 7
Соматические сенсорные нервы происходят в рецепторы в пенис, чтобы передать боль, температура, сенсорные и вибрационные ощущения, и мозг модулирует позвоночника пути возведения через медиальной преоптической области и паравентрикулярном ядра гипоталамуса, околоводопроводное серое вещество среднего мозга, а ядро paragigantocellularis из medulla.3 во время сексуального возбуждения, NO высвобождается из полового члена кавернозных нервных окончаний и эндотелия, диффундирует в трабекулярной и артериальных клеток гладкой мускулатуры, чтобы активировать гуанилатциклазы, таким образом катализировать образование вторичного мессенджера циклического гуанозин monophasphate (цГМФ). ЦГМФ в свою очередь активирует протеинкиназу г, фосфорилирования калиевых и кальциевых каналов; Конечным результатом является гиперполяризация, снижение intracytosolic кальция и диссоциация головки миозина действовать так гладко, мышца расслабляется. Циклическая adenosinemonophosphate (цАМФ) является еще одним вторичным посредником участвует в релаксации гладкой мускулатуры и активируется цАМФ - сигнальных молекул, включая аденозина, кальцитонин пептидов генных связанных и prostaglandins.4
|
|
С другой стороны, норадреналин, фенилэфрин и эндотелин -видимому, активируют фосфолипазу С, что приводит к образованию инозиттрифосфата и диацилглицерина. Конечным результатом увеличивается цитоплазматический кальций и последующее сокращение гладкой мускулатуры. Детумесценция происходит следующее деградацию цГМФ и цАМФ в GMP и AMP, соответственно, конкретных фосфодиэстеразы. Симпатическая разряд происходит, если результаты сексуальной стимуляции в ejaculation.8, 9 активированных Ро- киназы фосфорилирует, тормозит нормативно субъединицы гладких мышц миозинфосфатазы, предотвращая дефосфорилирование миофиламентов и поддержание сократительной tone.10 В спокойном состоянии, эти гладкие мышцы тонически контракт из-за внутренней тоном гладкой мышцы, адренергической разряда и других сигнальных молекул, таких как endothelin.4
Strength of the Evidence
Erectile dysfunction is a complex condition related to psychosocial and biological factors. It is difficult to reliably document and measure the degree of treatment success in patients diagnosed with this condition. Most of the validated and clinically relevant efficacy outcomes assessed in clinical trials of ED patients are subjective.
The strength of evidence regarding the utility of routine endocrinological blood tests found in this review was limited in terms of the both amount and quality of data. The studies were heterogeneous with respect to patient population characteristics, diagnostic methods, estimates of prevalence, and laboratory methods used (e.g. cut-off values, total, free, or bioavailable hormonal levels).
The placebo-controlled randomized trials that evaluated the efficacy and harms of PDE-5 inhibitors provided large amount of evidence and consistently indicated that patients who received PDE-5 inhibitors experienced greater improvements in erectile dysfunction compared with placebo-treated patients. The magnitude of benefit was clinically relevant and statistically significant. The methodological and reporting quality of the evidence provided by these trials was better than that for other studies (e.g. trials with active control arms or trials evaluating sublingual apomorphine, injections, topical, hormonal, or off-label therapies). Most of these trials enrolled ED patient populations with a broad spectrum of etiologies or comorbidities and assessed the same set of clinically relevant and validated outcome measures. Given the reported exclusion criteria for these trials, their results may not be readily applicable to ED patients with major chronic disorders (e.g. cancer, CVD, diabetes, psychiatric disorders, hepatic or renal diseases) or post-surgery patients, because the magnitude of clinical benefit conferred by PDE-5 inhibitors in such patients is relatively modest.384–386 Furthermore, vardenafil trials may have been comprised of more responsive patients due to the fact that about half of these trials excluded patients refractory to prior sildenafil therapy, thereby limiting the applicability of the results to a broader population of ED patients. On average, trials that evaluated injected (e.g. intracavernosal, subcutaneous), intra-urethral, topical, or other treatments were of relatively lower methodological and reporting quality.
|
|
A common limitation of these trials was a failure to assess and/or report clinically relevant treatment efficacy outcomes used for the measurement of the degree of erectile dysfunction (e.g. mean scores for International Index of Erectile Function, Sexual Encounter Profile, Global Assessment Question regarding improved erection). The most commonly assessed efficacy outcomes in these trials were penile rigidity (using RigiScan) and the quality of erections achieved at home. The trials did not report information on the methods used for randomization, blinding, and allocation concealment. Many study results may have been biased in favor of active treatment, because the analyzed samples predominantly included responders and excluded many randomized participants from their efficacy analyses. There was substantial heterogeneity across the hormonal treatment trials with respect to the diversity of patient populations (variations in inclusion/exclusion criteria; not all patients had ED), treatment interventions (type of intervention, mode of administration, dose, dosing regimen, duration), and the assessed outcomes.
In general, the reporting of harms was less consistent and detailed than that of efficacy outcomes. For example, the occurrence of any or serious adverse events was not reported in many trials. The definition of a serious adverse event may have varied across the trials. Some trials reported only most frequently encountered or treatment-related adverse events, the ascertainment of which may be prone to subjective judgment. In some instances, it was not explicitly defined whether the number and percentage referred to the actual number of adverse events or to the number of patients with at least one adverse event. In open label trials, patients or investigators may have over- or under-reported the incidence of adverse events because of their knowledge of the assigned treatment. Moreover disease-specific complications in patients with comorbidities and/or disorders known to cause ED could have been overlooked. In many cases, the statistical test results for between-group differences in adverse events were not reported, thereby limiting the interpretability of the data.
The reviewed evidence indicated that there is a lack of long-term efficacy and harms data associated with treatments for ED. This is especially important in the case of oral PDE-5 inhibitors and associated harms, given their prevalent use by men in the Western world (e.g. 7 percent of American men aged 56–65 years in 2002).30 Overall, duration of followup for the majority of reviewed trials was not sufficient to permit the reliable assessment of long-term (>6 months) treatment-related outcomes in patients with ED. The duration of followup for many of the PDE-5 inhibitor trials did not exceed 12 weeks. The long-term safety data obtained from retrospective observational studies is not as conclusive as that obtained from well-conducted long-term large randomized trials, which have fewer methodological limitations.
The reviewed evidence consisted of randomized trials using either parallel-arm or crossover design. Although crossover trials are efficient in terms of resources and study power, they require additional caution and careful interpretation of results. For example, one problem inherent in all crossover trials is a potential for a carryover effect, which could be minimized by employing an adequate washout period between alternative treatment periods.387 Although most of the authors reported the duration of washout periods (about 1–2 weeks), it is not clear what minimum length of time would be sufficient to avert or minimize carryover effects from the different types of treatment in patients with ED.
|
|
Утилизация и расходы, относящиеся к лечению ЭД
По оценкам Национального обследования здоровья и питания Экспертиза (NHANES) предполагает, что стоимость лечения ЭД в США может достичь 15 миллиардов долларов, если все люди стремились care.29 Анализы на дисфункции подгруппе эректильной для болезней урологических в Америке проекта установлено, что почти 1,5 процента приватно обеспечили мужчин в возрасте от 18 до 64, по крайней мере 1 претензии, связанные с ЭД в 2002 году; переключение формы медицинской помощи были продемонстрированы, как использование диагностических тестов для основных причин ЭД заметно уменьшилось и использование фармакологической терапии, особенно с оральных ингибиторов ФДЭ-5, increased.29
Данные Национального аптека претензий указано повышенную распространенность силденафила использования с 1,5 процентов в 1998 году до 2,9 процента в 2002 году, с его использование увеличивается с возрастом. Например, в 2002 году, 6 процентов мужчин в возрасте 55 лет и старше имели один или несколько пунктов формулы изобретения для sildenafil.30Furthermore, Департамента по делам ветеранов (VA) указал на девять -кратное увеличение для лечения ЭД между 1999 и 2003, с 9,3 процента мужчин 55-64 лет из отчетности возрастной автозаправочных рецепт на пероральных препаратов в 2003,29 общее использование медикаментозного лечения ЭД увеличилась с 17458 / 100000 в 1999 году до 56 716 / 100 000 в 2003,29 Это находит отражение в данныхВ.А. Аптека Преимущества группу управления, как предписания для конкретных ED препаратов увеличилась с 681/100, 000 до 6120 / 100000 в течение этого period.29 по национальных продаж, в 2005 году, фармацевтические затраты Силденафил, скачать, и варденафила были $ 1,6 млрд., $ 747 млн и $ 327 млн , respectively.31 -33
Силу доказательств
Эректильная дисфункция это сложное состояние, связанные с психосоциальных и биологических факторов. Трудно достоверно документировать и измерить степень успеха лечения больных с диагнозом этого заболевания. Большинство проверенных и клинически значимых показателей эффективности начисленных в клинических испытаниях пациентов ED субъективны.
Сила доказательств относительно полезности рутинных эндокринологических анализов крови, найденных в этом обзоре было ограничено с точки зрения как количества и качества данных. Исследования были неоднородны по отношению к пациенту характеристик населения, методов диагностики, оценки распространенности и лабораторных методов, используемых (например, пороговые значения, всего, свободный, или биодоступных гормональные уровни).
В плацебо-контролируемых рандомизированных исследований, в которых оценивали эффективность и вред от ингибиторов ФДЭ-5 при условии, большое количество доказательств и последовательно показали, что пациенты, которые получили ингибиторов ФДЭ-5 испытали большие улучшения в эректильной дисфункции по сравнению с плацебо лечение больных. Величина пользу было клинически значимых и статистически значимым. Методологическая и отчетности качество доказательств, представленных этих испытаний было лучше, чем, что для других исследований (например, испытаний с активными контроля над вооружениями или исследований, оценивающих сублингвально апоморфин, инъекции, местного, гормональные или не по прямому терапии). Большинство из этих исследований поступил ED групп пациентов с широким спектром этиологии или сопутствующих заболеваний и оцениваться тот же набор клинически значимых и проверенных мер результата. Учитывая заявленные критерии исключения для этих испытаний, их результаты не могут быть легко применимы к ЭД у пациентов с основных хронических заболеваний (например онкологических, сердечно-сосудистых заболеваний, диабета, психических расстройств, печеночной или почечной болезни) или послеоперационных больных, так как величина клиническая преимущество, предоставленное ингибиторов ФДЭ-5 у таких больных относительно modest.384 -386 Кроме того, варденафила испытания могут быть состоит из более чувствительных пациентов из-за того, что около половины этих испытаний исключались пациенты огнеупорных предварительного силденафила терапии, тем самым ограничивая применимость результатов к более широкой популяции больных ЭД. В среднем, испытания, которые оцениваются вводимые (например интракавернозную, подкожное), внутри- уретры, актуальным или другие виды лечения были относительно низкого методологического и отчетности качества.
Общее ограничение этих испытаний был провал для оценки и / или отчет клинически значимых результатов эффективности лечения, используемые для измерения степени эректильной дисфункции (например, средней оценки за Международного индекса эректильной функции, полового акта Профиль, Глобальная оценка вопрос относительно улучшилось монтаж). Наиболее часто оценивали результаты эффективности в этих испытаниях были полового члена жесткость (с использованием RigiScan) и качество эрекции, достигнутых в домашних условиях. Испытания не сообщают информацию о методах, используемых для рандомизации, ослепления и скрытого отнесения. Многие результаты исследования могут быть смещены в пользу активного лечения, так как анализируемые образцы преимущественно включены реагирования и исключить многие рандомизированных участников из их анализа эффективности. Был существенное неоднородность через гормональных исследований лечения по отношению к разнообразию групп пациентов (изменения в критерии включения / исключения; не все пациенты имели ЭД), лечебные меры (тип вмешательства, способа введения, дозы, режим дозирования, длительность), и начисленные результаты.
В целом, отчетность из зол было менее последовательны и подробно, чем из показателей эффективности. Например, возникновение любых или серьезных побочных эффектов не сообщалось во многих исследованиях. Определение серьезного неблагоприятного события, возможно, варьировалась в зависимости от испытаний. Некоторые исследованиях сообщалось только наиболее часто встречающихся или связанных с лечением нежелательных явлений,установление которого могут быть склонны к субъективности оценок. В некоторых случаях было явно не определено ли называют фактическим количеством побочных эффектов, либо числа пациентов количество и процентное содержание по крайней мере одной побочной реакции. В открытой испытания этикеток, пациенты или следователи могут иметь более или занижены частоту неблагоприятных событий в силу их знаний назначенного лечения. Осложнения Кроме того конкретным болезням у пациентов с сопутствующими заболеваниями и / или нарушений, способных вызывать ЭД, возможно, вышли. Во многих случаях статистические результаты тестирования различий между группами в неблагоприятных событий не сообщалось, тем самым ограничивая интерпретируемость данных.
Отзывы факты свидетельствуют о том, что существует нехватка долгосрочной эффективности и данных вреда, связанного с лечения ЭД. Это особенно важно в случае пероральных ингибиторов ФДЭ-5 и связанных с ними вреда, учитывая их преимущественное использование мужчинами в западном мире (например, 7 процентов американских мужчин в возрасте 56-65 лет в 2002 году).30 В целом, продолжительность катамнестического для большинство обзор исследованиях было недостаточно, чтобы разрешить надежную оценку долгосрочных (> 6 месяцев) результаты лечения, связанных у пациентов с ЭД. Продолжительность катамнестического для многих ингибиторов испытаний ФДЭ- 5 не превышает 12 недель. Данные долгосрочные безопасности, полученные из ретроспективных наблюдательных исследований не так убедительны, как полученное в результате правильно проведенных долгосрочных крупных рандомизированных исследований, которые имеют меньше методологические ограничения.
Отзывы доказательств состояла из рандомизированных исследований с использованием либо параллельно руку или дизайн кроссовера. Хотя кроссовер испытания являются эффективными с точки зрения ресурсов и исследования власти, они требуют дополнительного осторожность и тщательного интерпретацию результатов. Например, одна проблема присуща всем испытаний кроссоверпотенциал для переходящего эффекта, который может быть сведено к минимуму применением достаточного периода вымывания между альтернативное лечение periods.387 Хотя большинство авторы сообщили продолжительность периодов вымывания (около 1-2 недели), пока не ясно, что минимальная продолжительность времени будет достаточно, чтобы предотвратить или свести к минимуму переходящих эффекты от различных видов лечения у пациентов с ЭД.
Clinical Practice
Evidence regarding accurate identification of men who would benefit from testosterone replacement therapy is scarce. Thus, there is no universally accepted method of identifying men with clinically relevant hypogonadism affecting erectile function and the implications of androgen status for erectile dysfunction and its treatments remains controversial.389 Given the current gaps in knowledge, the most adequate and cost-effective laboratory test for hormonal evaluation is unclear. This problem is reflected in two differing guideline statements.14, 39 The American Urological Association recommends testosterone testing based on initial clinical assessment results or failure of prior management with PDE-5 inhibitors,14, while the European Urological Association mandates testosterone measures (bioavailable or calculated-free testosterone begin preferred over total levels) for all men with ED.39 These two groups have similar guidelines, which suggest that further endocrinological laboratory investigations including prolactin, LH, and FSH testing are indicated when low testosterone levels are detected. Optimal approaches from a clinical and resource-allocation standpoint remain to be determined. Regardless of the results, clinicians need to direct their initial efforts towards correctly identifying and treating, if possible, an underlying cause of ED, whether it is an endocrine or non-endocrine cause.
Apomorphine Versus Placebo
Efficacy. Overall, results from the five placebo-controlled trials indicated statistically significant improvements with respect to measures of erectile function (e.g. mean percentage of successful intercourse attempts, percentage of attempts resulting in erections firm enough for intercourse, rigidity ≥40 percent, and the mean IIEF “Erectile Function” domain score) in patients treated with apomorphine compared with those who received placebo. Clinically significant differences were seen in the mean percentage of improved erectile function with apomorphine compared with placebo arms.
Harms. There was insufficient information on the occurrence of any adverse events in these trials to allow comparison of incidence of harms across apomorphine and placebo groups. Adverse events such as nausea, headache, dizziness, and yawning occurred more frequently among patients who received apomorphine than among those who received placebo. The results from two trials suggested that the use of apomorphine was not associated with an increased incidence of any serious adverse events compared with the use of placebo.248, 250
Intracavernosal Injections
Prostaglandin E1 (PGE1)
Efficacy. The administration of PGE1 was shown to have improved erections more frequently relative to no treatment, placebo,papaverine, moxisylate, linsidomine, sodium nitroprusside, or the combination of linsidomine and urapidil. The rates of improvement in erection for patients receiving PGE1, sexual therapy, or the combination of papaverine plus phentolamine were found to be similar. Patients who received PGE1 alone experienced rates of improved erection similar to those among patients who received papaverine combined with phentolamine, while improved erection was less frequent after treatment with PGE1 plus papaverine. Limited detailed evidence suggests that trimix was at least as effective as PGE1 alone. Compared with trimix alone, the combination of trimix and sodium bicarbonate improved erections, while trimix combined with atropine did not produce such benefit. The interpretation of results from trials using trimix is complicated, because concentrations of the three constituents varied from study to study.392
Harms. Penile pain occurred more frequently in patients treated with PGE1 than among those treated with placebo, moxisylate, or the combination of papaverine and phentolamine. The pain associated with the treatment was significantly less frequent when the PGE1 was injected slowly, or in combination with either lidocaine or procaine, but not when injected in combination with sodium bicarbonate. The combination of papaverine and phentolamine was less frequently associated with pain in comparison with either PGE1 alone or PGE1 plus papaverine. The treatment with trimix was associated with priapism more frequently relative to treatment with PGE1. The variation in rates of priapism may additionally depend on proper testing of the agent in the office setting, dose adjustment process for use at home, teaching sessions during which the patient administers his own injection under supervision, patient compliance, instruction handouts, and/or missed injections.
Subcutaneous Injections
Intraurethral Suppositories
Alprostadil
Efficacy. The use of IU alprostadil was shown to be associated with a higher sexual intercourse success rate compared with placebo.
Harms. Patients receiving IU alprostadil had an increased risk of local pain compared with those who received placebo. The followup period of the trials did not exceed 3 months, so the relative benefits and harms of long-term treatment with IU suppositories remain unclear.
Topical Treatments
Hormonal Treatments
Testosterone
Efficacy. The effectiveness of testosterone regarding to improve erectile function and sexual intercourse satisfaction was inconsistent compared with placebo. Differences in patient inclusion criteria (e.g. not all trials were comprised of exclusively of ED patients), methods of evaluation, interventions (e.g. mono versus combination treatment, cream, patch, gel, injections), outcome definitions, and use of subjective measures (e.g. IIEF, SEP), could explain some of the discrepancies in results across the studies evaluating the efficacy of testosterone. The intramuscular administration of testosterone was shown to have improved erectile function compared with placebo in only one of four small trials. The “patch” testosterone did not improve sexual function compared with placebo. However, in men with poor response to previous use of sildenafil, testosterone patch plus sildenafil significantly improved the sexual intercourse success rate and satisfaction compared with placebo and sildenafil alone. Gel testosterone (50 mg and 100 mg doses) was found to have increased sexual intercourse frequency compared with placebo. The 100 mg dose of gel testosterone also significantly improved sexual intercourse frequency versus patch testosterone. The use of combination cream of testosterone, isosorbide dinitrate, and co-dergocrine was associated with an increased rate of successful sexual intercourse and improved erections compared with placebo or cream testosterone alone. The application of dihydrotestosterone gel was related to an increased rate of successful sexual intercourse compared with that of placebo.
Although there is insufficient head-to-head data, the gel formulation of testosterone may be a more effective treatment compared with other formulations of testosterone.
Harms. Patients receiving testosterone patch had a higher rate of having application site skin reactions than those with placebo. The use of gel testosterone did not show a dose-related increase in adverse events. The use of combination cream containing testosterone, isosorbide dinitrate, and co-dergocrine was associated with an increased risk of mild headaches compared with placebo or cream testosterone alone. The short-term followup precluded ascertainment of the incidence of prostate cancer. In one trial,317 two patients who had been treated with patch testosterone, developed prostate cancer.
Phentolamine
Efficacy. The results indicated either numerical or statistically significant improvements in erectile function (i.e., percent of successful intercourse attempts, base/tip rigidity >60 percent for ≥ 10 minutes) were associated with the use of phentolaminerelative to placebo. There was no between-group difference for tumescence activity units.333 With insufficient data, statistical test results, and a small number of studies, the trial results are inconclusive regarding the efficacy of phentolamine relative to placebo.
Harms. Due to the lack of sufficient amount of harms data it is not clear if patients taking oral phentolamine are at higher risk of developing adverse events.
Trazodone
Efficacy. Evidence regarding efficacy of trazodone relative to placebo to treat ED was insufficient (i.e., only 5 smaller-scale trials) and inconsistent. In general, the use of trazodone was not associated with improved erectile function compared with placebo.336,337, 339, 341 Note that in one trial,344 patients on trazodone experienced statistically significant improvement in erectile response (i.e., at least 3 successful intercourses within 30 days of treatment) compared with those on placebo, ketanserin, or mianserin. Since this trial was not double blind, it is hard to judge if the observed differences were truly due to the treatment administered or to other extraneous factors. The current American Urological Association Practice Guidelines Committee (AUA PGC) does not recommend the use of trazodone in the treatment of ED.14
Harms. Limited evidence suggests that the use of trazodone may be associated with an increased risk of adverse events (priapism, sedation, headache) and higher rates of withdrawal due to adverse events compared with placebo.
Cabergoline
Efficacy. The limited amount of evidence suggests that the use of cabergoline was associated with numerically or statistically significantly improved mean scores of IIEF “EF” domain and IIEF-Q3/Q4 compared with placebo. Additional evidence from trials using different doses is needed to corroborate or disprove these findings.
Harms. In general, treatment with cabergoline was well tolerated. Nevertheless, there were higher frequencies of adverse events and withdrawals due to adverse events in the active treatment groups than in the placebo groups.
Pentoxifylline
Efficacy. The results of the trials were inconsistent, one340 indicated statistically significant improvements in peak systolic velocity; and the other trial343 yielded no difference in the frequency of morning erections, nocturnal penile tumescence, or penile rigidity in patients receiving pentoxifylline compared with those on placebo. Another trial345 demonstrated an increased number of successful coital episodes for the active treatment group of patients. However no formal statistical test results were presented to substantiate the findings. Given the above-mentioned limitations, more evidence is needed to draw more definitive conclusions regarding the relative efficacy of pentoxifylline.
Harms. No harms data were reported for two trials.343, 345 Some of the reported treatment-related adverse events in one trial340were nausea and headache. The harms profile of pentoxifylline in treating ED remains unclear.
Miscellaneous Agents
Efficacy. Overall, the limited amount of evidence suggested that naltrexone, tianeptine, tetrahydrobiopterin, and dehydroepiandrosterone may be more efficacious than placebo in improving early morning erections, proportion of patients with successful intercourse attempts, duration of rigidity (>60 percent), and mean total IIEF domain-specific scores, respectively.342,348, 352, 353 The evidence regarding the efficacy of moclobemide, isoxsuprine, angiotensin-converting enzyme (ACE), and myoinositol/folic acid was less conclusive.334, 335, 346, 351 The degree of erectile response was not statistically significantly different for isoxsuprine or ACE relative to placebo.335, 346 Although moxonidine was shown to be more effective in increasing deep penile diameter and artery velocities compared with metoprolol, this result may have been biased because this trial did not employ double blind techniques to adequately mask the treatment modality.347 More trials using a double-blind design are needed to corroborate these findings.
Harms. The limited amount of evidence suggested that the number of patients with adverse events was greater in the treatment groups than in the placebo groups. No definitive conclusions can be made at this time.
Origin of ED
There was a consistent clinical benefit (i.e., IIEF “EF” domain and GAQ-Q1) in patients receiving sildenafil, tadalafil, or vardenafilcompared with placebo regardless of their origin of ED (i.e., organic, psychogenic, and mixed). This suggests that quite a broad etiologic spectrum of ED patients could potentially benefit from using these agents to improve the clinical symptoms of ED. This review of evidence did not reveal the presence of any obvious treatment effect modification by the origin of ED. However, these results were obtained from only a few trials, so the evidence warrants a cautious interpretation. Additional trials conducted in these subgroups using uniformly defined clinical outcomes would help to draw more definitive conclusions.
Baseline Severity of ED
The use of PDE-5 appeared to elicit a better improvement in erectile function (i.e., higher endpoint scores on IIEF “EF domain,” IIEF-Q3/Q4, GAQ-Q1) for patients with mild or moderate baseline severity of ED (IIEF score: 11–25) than for those with severe forms of ED (IIEF score ≤ 10).
Duration of ED
There is a paucity of evidence on the relative efficacy of PDE-5 inhibitors according to the duration of ED. Only a few trials (i.e.,sildenafil versus placebo) reported the efficacy analysis stratified according to the duration of ED with consistent clinical benefits for all patients irrespective of the duration of ED. Furthermore, the two trials in diabetic men with ED94, 101 did not reveal any trends in efficacy (IIEF-Q3/Q4 and GAQ-Q1) across the ED duration strata. The evidence is still inconclusive whether or not the duration of ED is an important prognostic factor for the degree of treatment success (e.g. endpoint IIEF “EF” domain scores, proportion of patients with IIEF >25 at followup).
Distinct Clinical Subgroups
Evidence on incremental therapeutic benefits associated with the use of PDE-5 inhibitors was consistent across a broad spectrum of patients with ED. The obvious clinical benefit of PDE-5 inhibitors relative to placebo in treating ED was observed not only in the trials that included a broad spectrum of patient population with ED but also in the trials restricted to specific clinically defined homogenous groups of patients with ED (e.g. diabetes, depression, prostate cancer, spina bifida, stable CAD, Parkinson's disease, CHF, LUTS, MS, renal transplants, arterial hypertension, prostatectomy, and no prior treatment for ED). The results of meta-analyses conducted for this review also showed that the use of sildenafil in patients with diabetes, depression, or hypertension led to improvements with respect to IIEF-Q3/Q4, GAQ-Q1, and percentage of successful intercourse attempts.
Conclusions
The evidence comparing cause-specific therapies with symptomatic treatments (e.g. PDE-5 inhibitors, injections, and hormonal treatments) for management of ED is lacking. Due to the complexity of causative and comorbid factors, more studies are needed to clarify the best treatment management options for various subgroups of patients with ED (e.g. endocrinopathies, concurrent clinical conditions). There is also a need for trials comparing PDE-5 inhibitors with other treatments for ED (e.g. oral, injected and topical). Long-term effects of ED treatments in RCTs have not been adequately explored. To clarify and determine the clinical utility of routine hormonal blood tests in ED patients, studies are needed in representative populations, with comparable diagnostic criteria and types of tests for hormonal disorders.
Выводы
Доказательства сравнения конкретных причин терапии с симптоматического лечения (например, ингибиторов ФДЭ-5, инъекции, и гормональные препараты) для управления ЭД не хватает. Из-за сложности причинных и сопутствующих факторов, необходимы дальнейшие исследования, чтобы уточнить наиболее эффективные варианты лечения лечение для различных подгрупп пациентов с ЭД (например эндокринопатии, одновременно клинических условиях). Существует также потребность в исследованиях, сравнивающих ингибиторов ФДЭ-5 с другими методами лечения ЭД (например оральный, вводят и местного). Долгосрочные эффекты ED лечения в РКИ не были должным образом изучены. Для уточнения и определить клиническую эффективность обычных гормональных анализов крови у больных ЭД, исследования необходимы в представительных населения, с сопоставимыми диагностических критериев и видов тестов для гормональных нарушений.
Definition of Erectile Dysfunction
Erectile dysfunction (ED) is defined as the persistent inability to achieve or maintain penile erection sufficient for satisfactory sexual performance.1 The 1992 National Institutes of Health (NIH) Consensus Development Conference recommended the use of erectile dysfunction as the preferred term to impotence, the former being more precise.1 There is no universal consensus or agreed criteria as to how consistent the problem (i.e., inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance) has to be and for what duration it should last to fulfill this definition. A period of persistence over 3 months has been suggested as a reasonable clinical guideline.1, 2
Physiology of Erection
Penile erection is a complex process involving interactions between neural, psychological, vascular, and hormonal factors. The pathway of normal sexual function in males consists of four stages: sexual desire (i.e., libido), erection, ejaculation (i.e., orgasm), and detumescence (penile flaccidity).3 The erection cycle is initiated by sexual stimulation. Erection subsides at ejaculation or cessation of sexual stimulation and the subsequent flaccidity state is maintained until the next sexual stimulation or nocturnal erection occurs. Thus, both the erection and the flaccidity states of the penis exist in two phases, initiation and maintenance. Pathways responsible for penile flaccidity are no less important than pro-erectile mechanisms, and may play critical roles in certain types of erectile dysfunction (ED).4 Additionally, hormones function not only at the libido level, but help maintain anatomical and physiological integrity of penile cavernosal structures; testosterone deficiency interferes not only with normal function, but can also diminish response to ED treatment.5
The mechanism of erection involves responses to external sensory stimuli through parasympathetic activity, which leads to release of nitric oxide (NO) from nonadrenergic-noncholinergic (NANC) cavernous (penile) nerve endings and the endothelium of the penis. The initial phase of smooth muscle relaxation results in reduced peripheral resistance of cavernosal arterioles and thereby allows blood to flow into the penis under the driving force of systemic blood pressure.4 Once blood rushes into the sinusoids of the corpora cavernosa, shear stress can also release NO from endothelium to augment smooth muscle relaxation and erection. In addition, oxygen tension and substances secreted by endothelium lining the sinusoidal spaces, (i.e. prostaglandins, endothelins, and angiotensin) may also be involved in penile erection and detumescence.6, 7
The somatic sensory nerves originate at receptors in the penis to transmit pain, temperature, touch, and vibratory sensations, and the brain modulates the spinal pathways of erection via the medial preoptic area and paraventricular nucleus of the hypothalamus, periaqueductal gray of the midbrain, and the nucleus paragigantocellularis of the medulla.3 During sexual stimulation, NO released from the penile cavernosal nerve endings and endothelium, diffuses into the trabecular and arterial smooth muscle cells to activate guanylyl cyclase, thereby catalyzing the formation of second messenger cyclic guanosine monophasphate (cGMP). The cGMP in turn activates protein kinase G, phosphorylating potassium and calcium channels; the end result is hyperpolarization, reduced intracytosolic calcium, and dissociation of the myosin head from acting as smooth muscle relaxes. Cyclic adenosinemonophosphate (cAMP) is another second messenger involved in smooth muscle relaxation and is activated by cAMP-signaling molecules including adenosine, calcitonin gene-related peptides, and prostaglandins.4
On the other hand, norepinephrine, phenylephrine, and endothelin appear to activate phospholipase C, leading to the formation of inositol triphosphate and diacylglycerol. The net result is increased cytoplasmic calcium and subsequent smooth-muscle contraction. Detumescence occurs following degradation of cGMP and cAMP to GMP and AMP, respectively, by specific phosphodiesterases. Sympathetic discharge occurs if sexual stimulation results in ejaculation.8, 9 Activated Rho-kinase phosphorylates, inhibits the regulatory subunit of smooth muscle myosin phosphatase, preventing dephosphorylation of myofilaments and maintaining contractile tone.10 In the flaccid state, these smooth muscles are tonically contracted due to intrinsic smooth-muscle tone, adrenergic discharge, and other signaling molecules such as endothelin.4
Определение эректильной дисфункции
Эректильная дисфункция (ЭД) определяется как устойчивая неспособность достигать или поддерживать эрекцию полового члена, достаточную для проведения коитуса.1 В 1992 Национальный институт здоровья (NIH) на конференции по развитию рекомендовал использовать термин «эректильной дисфункции» в качестве более предпочтительного вместо импотенции.1 На тот момент не существовало согласованных критериев относительно того, как сформировать проблему (т.е. неспособность достигать или поддерживать эрекцию полового члена, достаточную для успешного полового акта) и как долго должна наблюдаться дисфункция чтобы соответствовать данному определению. Период в течение 3 месяцев был предложен в качестве наиболее разумного.1, 2
Физиология эрекции
Эрекция полового члена представляет собой сложный процесс, включающий взаимодействие между нервной системой, сосудистой системой, гормональных факторов и психологических аспектов. Нормальная сексуальная функция мужчины состоит из четырех этапов: сексуального желания (т.е. либидо), эрекции, эякуляции (т.е., оргазма), и детумесценции.3 Данный цикл инициируется сексуальной стимуляцией. Эрекция прекращается после эякуляции или прекращения сексуальной стимуляции с последующим поддерживающимся состоянием детумесценции, пока не произойдет следующая сексуальная стимуляция или ночная эрекция. Таким образом, и состояния эрекции и состояние вялости полового члена осуществляются в два этапа: инициирования и поддержания. Не Пути, ответственные за полового члена вялости не менее важны, чем про- эректильной механизмов, и может играть решающую роль в некоторых видах эректильной дисфункции (ЭД) 0,4 Кроме того, гормоны функционировать не только на уровне либидо, но поможет сохранить анатомическую и физиологическую целостность полового члена кавернозных структур; дефицит тестостерона препятствует не только с нормальной функцией, но также может уменьшить ответ на ED treatment.5
Механизм эрекции предполагает ответов на внешних сенсорных стимулов через парасимпатической активности, что приводит к высвобождению оксида азота (NO) из неадренергических - нехолинергических (NANC) кавернозных (полового члена) нервных окончаний и эндотелия пениса. Начальная фаза гладких результатов расслабления мышц в сниженной периферической сопротивления кавернозных артериол и тем самым позволяет крови течь в пенис под движущей силой системного pressure.4 крови После кровь приливает в синусоиды кавернозных тел, напряжение сдвига может также освободить НЕТ от эндотелия, чтобы увеличить расслабление гладкой мышцы и эрекцию. Кроме того, напряжения кислорода и веществ, выделяемых эндотелия, выстилающих синусоиды пространства, (т.е. простагландины, Эндотелины и ангиотензина) также могут быть вовлечены в эрекции полового члена и detumescence.6, 7
Соматические сенсорные нервы происходят в рецепторы в пенис, чтобы передать боль, температура, сенсорные и вибрационные ощущения, и мозг модулирует позвоночника пути возведения через медиальной преоптической области и паравентрикулярном ядра гипоталамуса, околоводопроводное серое вещес<
|
|
|
Организация стока поверхностных вод: Наибольшее количество влаги на земном шаре испаряется с поверхности морей и океанов (88‰)...
Археология об основании Рима: Новые раскопки проясняют и такой острый дискуссионный вопрос, как дата самого возникновения Рима...
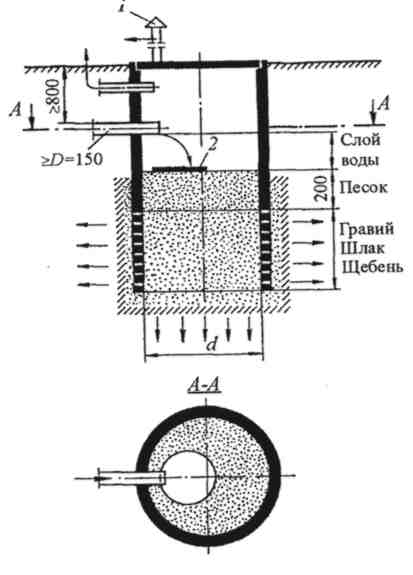
Индивидуальные очистные сооружения: К классу индивидуальных очистных сооружений относят сооружения, пропускная способность которых...
История создания датчика движения: Первый прибор для обнаружения движения был изобретен немецким физиком Генрихом Герцем...
© cyberpedia.su 2017-2024 - Не является автором материалов. Исключительное право сохранено за автором текста.
Если вы не хотите, чтобы данный материал был у нас на сайте, перейдите по ссылке: Нарушение авторских прав. Мы поможем в написании вашей работы!