Duodenal intubation
This examination of duodenal material is carried out for the purpose of determining both normal components (bile, enzymes of pancreatic juice) and pathological (leucocytes, microbes, various parasites) (Fig.31).
A special tube not less than 1,5 m long, with 3 circular marks, 50, 70, 90 cm from the introduced end, is used for intubation. At the end of the tube there is a metal terminal bead with a lot of openings running to the internal canal.
Intubation is carried out on an empty stomach in a sitting position. The terminal bead is placed deeply on the tongue root, and the patient swallows it. With the help of active gulps the tube moves down to the stomach. To prevent vomiting the patient is asked to breathe deeply. When the terminal bead has passed the gullet and is in the stomach (the first mark on the tube - 50 cm), the patient is in right lateral decubitus without a pillow and with the help of a syringe the stomach contents is sucked out. Peristaltic motions of the stomach move the terminal bead of the tube forward into duodenum to the second mark on the tube (70 cm). A hot-water bottle is placed on the area of liver and a bolster is put under the patient, so that the underpinning is raised. In this position the patient slowly swallows the tube to the third mark (90 cm) within 20-30 minutes. The free end of the tube is put into a test tube. The test tube support is set on a low bench at the patient’s bed-side. After the terminal bead gets into duodenum, bile starts coming out of the tube – yellow liquid of alkaline reaction. If the terminal bead stays long before the pylorus, the patient is given 30 ml of 10 % warm solution of sodium carbonate to drink.
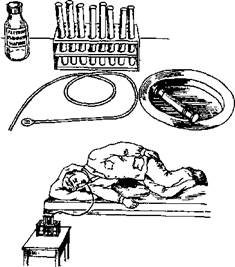
Fig.31. Duodenal intubation
Intubation can be carried out by two methods: classic three-phase method and multiple (fractional).
Three-phase method
Phase 1 – extraction of portion A (duodenal bile). Duodenal bile comes out by itself. Usually 15-40 ml of clear, golden-yellow bile is collected during 20-30 minutes.
Phase 2 - extraction of a portion B (cystic bile). For this purpose it is necessary to cause opening of Oddi's sphincter and constriction of gall-bladder. This is achieved by introducing gall-bladder constriction activators through the tube: 33 % of solution of magnesium sulfate, 10 % of solution of sorbite. It is possible to introduce cholecystokinin (75 units into 10 ml of isotonic solution of sodium chloride intravenously) or pituitrin (5 units intramuscularly), which cause significant constriction of gall-bladder. After introducing the activator the tube is pressed with a clamp for 2-3 minutes, then the clamp is removed and cystic bile is collected. Bile of portion B is thick, of dark-olive (brown) color, clear, is excreted freely during 20-30 minutes; during this time 50-60 ml of bile is collected.
Phase 3 - extraction of portion C (hepatic bile). Gradually cysticbile starts to grow light and becomes of golden-yellow color. This portion is excreted from hepatic ducts. Duration of excretion – 20-30 minutes, amount – 15-20 ml. After having collected portion C the tube is removed.
Fractional method
After introducing the tube into the duodenum 5 fractions of bile corresponding to certain phases of biliary excretion are extracted.
Phase 1 – time of common bile duct – begins from the moment when the tube is introduced into the duodenum and lasts till introduction of the activator. If the person is healthy, this phase proceeds 20-30 minutes, during this time 15-40 ml of golden-yellow bile is excreted.
Phase 2 – of closed Oddi's sphincter – from the moment the activator is introduced of till a new portion of golden-yellow bile comes out of the tube. Normally this phase lasts 4-6 minutes.
Phase 3 – excretion of golden-yellow contents of the cervical duct and gall bladder neck. Duration of the phase – 3-4 minutes, 3-5 ml of bile is collected.
Phase 4 – extraction of cystic bile, begins when dark brown cystic bile comes out. Normally 30-60 ml of bile is collected during 20-30 minutes.
Phase 5 – extraction of hepatic bile, begins when golden-yellow bile comes out of hepatic ducts and liver. 15-20 ml of bile is collected during 20-30 minutes. After phase 5 finishes, the tube is removed.
Anatomico-physiological peculiarities of constitution of intestinal tract
The intestinal tract is 7-8 m long and consists of two parts: the small intestine (duodenum, jejunum and ileum) and the large intestine (caecum with vermiform appendix, segmented intestine, sigmoid and rectum). At the border of the small and large intestines there is an ileocolic valve. At the end of rectum there is a sphincter muscle of anus.
The main functions of the intestinal tract are digestive, absorbing and motor. The process of digestion in the intestinal tract takes place under the influence of pancreas secretion, bile, intestinal juice and ends by formation of substances that can be absorbed. Bacterial flora of the intestinal tract takes part in intestinal digestion and formation of some vitamins.
Absorption of amino acids, monosaccharides, fatty acids and soaps takes place in the small intestine and in the large intestine only water is absorbed. Motor function of the intestinal tract mainly consists in pendular movements, due to which food is mixed, and peristaltic motions that move the intestinal material forward to the large intestine. Movement of material in the small intestine lasts 3-4 hours, in the large intestine – 17-24 hours.
The main symptoms of diseases of intestinal tract and first aid in case of such
Intestinal colic – short, frequent, suddenly beginning (cramping) episodes of pain that are felt in different parts of the intestinal tract, accompanied by tympania and are relieved after passage of flatus. A special kind of intestinal colics are tenesmi – painful and frequent desire for stool with excretion of a small amount of slime, which is evidence of inflammatory process in the rectum (dysentery).
In case of pains in the stomach it is prohibited to take anaesthetics and apply hot-water bottle until the doctor finds out the cause of pains, as these interventions can complicate the diagnostics and even harm the patient.
Diarrhea results from disorder of motor and secretory functions of the intestinal tract. Irritation of intestinal mucosa causes hyperperistalsis, and the remains of not yet digested and absorbed food quickly move forward in the intestinal tract and leave it. If thus there is intestinal mucositis, then in fluid excrements there are various foreign matters.
In case of inflammation of the small intestine (enteritis), excrements are fluid, profuse, yellow-green in color, 3-6 times a day. In case of inflammation of the large intestine (colitis), the stool is more frequent, up to 15 times a day, in small portions with slime and blood.
Patient care consists, first of all, in keeping their body, bed clothes and linen clean. The patient should use not the toilet but bedpan or a chamber-pot, so that the doctor can examine the feces. After each defecation the anus area of patients should be washed with a weak disinfectant solution.
Diarrhea is often a sign of infection, therefore those giving care are obliged to carry out current disinfection until its cause becomes known.
1. It is necessary to allocate a room or a light part of the common room for the patient with a separate bed and bedding, without unnecessary things, leaving in it only necessary things, to put a rug wetted in a disinfectant solution on the threshold.
2. Plates and dishes of such patients should be separate, it is necessary to store and wash it separately from other plates and dishes in hot water with soap and soda and to boil it during 15 minutes once a day.
3. The patient’s feces and urine in the chamber-pot should be filled up with dry bleaching powder in the ratio 1:2 for one hour, and then poured out into the sewerage system. The remains of food are disinfected in the same way.
4. After disinfection the individual chamber-pot or bedpan should be kept on a special bench or on a sheet of paper which is frequently changed. Dirty paper should be burnt.
5. Objects of patient care are to be cleansed daily by washing and boiling for not less than 15 minutes.
6. The patient’s dirty linen should be collected separately into a closed tank and boiled for 15 minutes in a soap-soda solution before washing. Linen dirty with feces is to be rinsed in wash water and filled up with dry bleaching powder leaving it for one hour.
7. Wet cleaning of the patient’s room and public places is to be done 2-3 times a day; floors are to be washed with hot water with soap and soda; door handles water-closet lid, w.c. pan and floor are to be wiped with a cloth wetted in a disinfectant solution. For this purpose it is necessary to have a separate bucket and floor-cloths, which are regularly specially cleansed and disinfected or boiled.
8. To combat flies who are distributors of infection.
9. Those looking after patients must wear an overall made of some easily washed fabric atop and strictly observe rules of personal hygiene:
А) After cleaning the room, disinfection of plates and dishes, giving the bedpan it is necessary to wash hands with soap and a brush carefully;
B) When going out of the ward, to remove the dirty overall and wipe the footwear with a disinfectant solution.
Constipation is a consequence of slowing down of defecation that results in rare defecation with a small amount of solid feces, sometimes scybalous stool. Constipation can arise without any disease of the intestinal tract, only as a result of wrong nutrition or starvation, dehydration of the organism or taking easily digestible food lacking vegetable fiber, etc.
Hypokinetic constipation appears as a result of weakness of intestinal muscles and when irritability of the intestinal wall is low; as well as in case of diseases of adjoining organs. In this case the intestinal contents stays in the left part of the large intestine from 24 hours to one week.
Hyperkinetic constipation often results from general neurosis with the prevalence of tonus of parasympathetic nervous system. As a result of retention of fecal masses in a certain section of the large intestine, putrefaction of albumens takes place in the superposed parts; this leads to intoxication and still stronger spasms.
Constipation can be caused by a mechanical obstacle in case of intestinal tract growth or abdominal cavity growth, in case of kinks, commissures, etc. in case of ileac passion there is retention of both fecal masses and gases.
Patients with strict confinement to bed may suffer from constipation because of lack of movements.
In case of constipation patients feel heaviness and distention in the stomach, pains, feel incomplete bowel emptying. Absorption of putrifaction products due to congestion of fecal masses in the intestinal tract causes poisoning of the organism, which is felt through headaches, languor, feebleness.
To control constipation laxatives and enemas are periodically given to the patient on the doctor’s prescription.
Patients suffering from hypokinetic constipation may have a significant accumulation of consolidated fecal masses in the rectum which must be taken out with fingers since in such cases enemas are not effective. For this purpose the bedpan is put under the patient, the nurse puts on rubber glove, greases fingers with vaseline and, introducing 1-2 fingers into the rectum, takes the feces out in parts, then gives a cleansing enema.
Fecal incontinence results from the disorder of nervous control of defecation, when the patient has diseases of nervous system, diseases accompanied by loss of consciousness (infections, cerebral hemorrhage, etc.). Rectal incontinence can be the consequence of local inflammatory, tumorous and traumatic diseases in area of the rectum sphincter.
Usually patients with fecal incontinence areplace in a separate ward. Nutrition of such patients must be high-calorific and easily digestible. Having satisfied the needs of the organism, such food gives minimum of remains for feces formation. Every morning the patient’s intestinal tract is emptied with the help of enema. Such patients periodically lie on a rubber bedpan or on a specially equipped bed and need constant care of cleanness of the body with the help frequent intimate washing, rubdown, changes of linen.
Tympania – distention of stomach when there is superfluous accumulation of gases in the intestinal tract and displays itself as arching pain in the stomach. Tympaniamore often troubles patients after abdominal operations and with diseases of peritoneum. In such state, firstly, a diet lacking carbohydrates is prescribed; secondly, 1 teaspoon of activated charcoal or Carbolenum tablets 2-3 times a day, camomile tea and other herbs are prescribed; thirdly, cleansing enemas are given, which help to remove both feces and gases from the intestinal tract, relieving the patient significantly. If enema is undesirable or distention remains after it, colonic tube 40-50 cm long with the diameter of lumen 5-10 mm, with a rounded end with two lateral openings is introduced. Having greased beforehand the end of the tube with vaseline, it is introduced into the rectum 20-40 cm deep, the external end is placed in the bedpan put under the patient. In one hour the tube is carefully removed, the anus is wiped with a wet cotton wool wad and greased with ointment (Fig.32).



Fig. 32. Use of the colonic tube:
А) Appearance of the colonic tube Б) introduction of the colonic tube С) removal of gases
Enterorrhagia arises in cases of ulceration of the gastrointestinal tract, dysentery, abdominal typhoid, disturbed circulation in the intestinal wall and hemorrhages caused by general diseases accompanied by bleeding sickness.
Common symptoms for such patients are: weakness, dizziness, sonitus, dyspnea, syncopal state, sudden skin blanching, rapid pulse of poor volume, fall of AP.
Appearance of excrements in cases of enterorrhagia is different depending on the place of the bleeding source and the speed at which blood moves in the intestinal tract. In cases of hemorrhage from duodenal ulcer, ingress of blood to the intestinal tract and gastrorrhagia the stool will be tarry since under the influence of hydrochloric acid of gastric juice hemoglobin has time to turn into black hematin while blood is moving in the intestinal tract. If the source of hemorrhage is lower, blood is less changed, and in case of hemorrhage from varicosed rectal veins if there is hemorrhoids or from anal fissures unchanged blood can be admixed to regular feces.
Patients with enterorrhagia must observe strict confinement to bed. It is possible to put an ice bag on the patient’s stomach (Fig.33). It is obligatory to urgently inform the doctor about the hemorrhage and to show the feces to him. In case of acute hemorrhage from stercoral ulcer patients are allowed neither to eat, nor to drink for 1-2 days, and then mechanically and chemically sparing diet (diet №1а) is prescribed. In case of hemorrhoidal bleeding it is necessary to control constipation.
On the doctor’s prescription haemostatics are used in the parenteral way.