
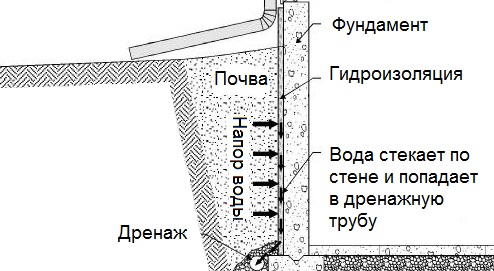
Общие условия выбора системы дренажа: Система дренажа выбирается в зависимости от характера защищаемого...
Состав сооружений: решетки и песколовки: Решетки – это первое устройство в схеме очистных сооружений. Они представляют...
Общие условия выбора системы дренажа: Система дренажа выбирается в зависимости от характера защищаемого...
Состав сооружений: решетки и песколовки: Решетки – это первое устройство в схеме очистных сооружений. Они представляют...
Топ:
История развития методов оптимизации: теорема Куна-Таккера, метод Лагранжа, роль выпуклости в оптимизации...
Комплексной системы оценки состояния охраны труда на производственном объекте (КСОТ-П): Цели и задачи Комплексной системы оценки состояния охраны труда и определению факторов рисков по охране труда...
Техника безопасности при работе на пароконвектомате: К обслуживанию пароконвектомата допускаются лица, прошедшие технический минимум по эксплуатации оборудования...
Интересное:
Берегоукрепление оползневых склонов: На прибрежных склонах основной причиной развития оползневых процессов является подмыв водами рек естественных склонов...
Что нужно делать при лейкемии: Прежде всего, необходимо выяснить, не страдаете ли вы каким-либо душевным недугом...
Отражение на счетах бухгалтерского учета процесса приобретения: Процесс заготовления представляет систему экономических событий, включающих приобретение организацией у поставщиков сырья...
Дисциплины:
|
из
5.00
|
Заказать работу |
|
|
|
|
Mouth cavity care
General care is performed daily (in the morning and evening) by cleaning the teeth with the help of a toothbrush. The nurse wipes the mouth of serious patients after each meal. Using tweezers or forceps she takes the cotton-wool wad wetted in 0,5% solution of borax and drawing aside the cheek with the help of a spatula she wipes all the teeth, gums, the tongue and oral mucosa with the cotton-wool wad.
To prevent xerochilia (dryness of lips) and fissures in the angles of mouth, the lips are smeared with butter or vaseline several times a day.
The nurse also observes nasal passages – free breathing through the nose prevents xerostomia. If there appear dry crusts in the nose, she puts a gauze trailer wetted in vaseline oil into the nasal passages or drips 1-2 drops of warm water.
Eyes care
If there appears puriform discharge in the corners of the eyes, the nurse must bathe them with a dilution of potassium permanganate or a solution of Furacilin (1:1000). To perform this the lower eyelid is pulled down with the left hand forefinger and a full pipette of the solution of room temperature is poured into the conjunctival sac in a squirt. The pipette used for the bathe must be sterile.
Giving a bedpan
Serious patients void physiological needs without getting up from bed, that is why he is to be helped without causing him unnecessary trouble and dirtying bed linen.
One of the items needed for attending patients is a bedpan, which can be of different shape and construction. It is made of faience, metal with enamel coating or rubber. Most often the bedpan is of flat round shape with a big round opening on top, which is covered with a lid, and with a small opening in the tube situated on the side surface and serving for discharge of the contents. A clean bedpan must stay under the bed on a small bench.
While using the bedpan, the patient must be separated from other patients by a screen. The bedpan is washed with warm water beforehand and some water is to be left in the bedpan. The nurse’s hand is put under the patient’s sacral bone, so the pelvis goes up and the bedpan is put between separated legs bent in knees. The bedpan is put under the buttocks so, that the perineum is above the big opening and the tube – between the hips.
Nutrition of Patients
Nutrition is a vital need of an organism. Human health depends on eutrophy in many respects. “Let your food be your first medicine!” – edified Hippocrates. Sensible nutrition science is called dietetics and a diet defines the dietary pattern, composition and amount of food. Diet therapy is nutritional care of the patient on treatment. Nutritional care is based on the doctrine of I.P. Pavlov who proved the necessity of timely meals, the importance of not only calorie content of food but also of appearance of food and even of the persons who serve meals. Nutrition should be regular, full, diverse and moderate. A healthy person should consume daily about 150 gr. of protein, 100 gr. of fat, 400-500 gr. of carbohydrates, 1500—2000 ml. of liquid, about 10 gr. of NaCl, necessary amount of К, Са, Fe, Мn, etc. and vitamins. Food ration should contain about 40-50 gr. of ballast agent – dietary fibres.
|
|
The organism’s need of food is regulated by appetite and the sense of satiety. Monotonous food suppresses the appetite even of a healthy man. The meals should be well-cooked, so that it is digested and assimilated well. In hospitals there should be four meals a day; in case of heart diseases and peptic ulcer – 5-6 meals a day at definite hours without hurry. The appearance and taste of food are very important. If there are no contra-indications to spices and kitchen herbs, they can be added to the patient’s food to make the taste better. The temperature of hot dishes should be about 60 оС, of cold – 10-15°С.
Nutrition in medical institutions has a therapeutic effect. Some patients are prescribed superalimentation (persons with emaciation, pregnant women and nursing mothers), others are recommended to go hungry (uncontrollable vomiting, peptic ulcer haemorrhage). Some patients are restricted in eating particular products, for example, fatty food in cases of diseases of gall bladder and liver, roughage and spicy food in cases of stomach diseases, table salt in cases of hypertension, kidneys diseases, liquids in cases of oedema.
Diet is a special ration and dietary pattern, drafted for the patient as a therapeutic method and a preventive measure against complications.
Dietary nurses and dietary doctors supervise nutrition in medical institutions. In the department the head nurse or the dietary nurse controls nutrition. Every day a special diet is drafted for all patients marking the number of the diet; the diet is signed by the chief of department and is passed on to the dietary doctor or nurse.
In the department there is a stillroom where the food is delivered centrally. The barmaid must keep containers with food in proper cleanness. Containers are put onto special mobile tables with a heating device and are delivered to the canteen or ward. Open ward patients dine in the canteen where there are tables for 2-4 persons. They are offered seats according to their dietary menu. After dinner the tables are removed, after supper they are washed with hot water and soap. Tableware is kept in the stillroom. After the food is given out it is passed on to the service hatch, where there are electric ovens for warming the food up. Here there are boilers for hot water and the washery. Food waste is kept in closed buckets or containers. In summer gauze is fixed on the windows to protect the food from flies. Cockroaches and flies in nutrition unit are evidence of its bad sanitary state. The dishes are washed twice with hot water and mustard or soda and it is obligatory that they are disinfected with 0,2% clear solution of chlorinated lime, rinsed in hot water and put into cupboard drier.
Nutrition of serious patients is carried out by medical personnel. Debilitated patients are put into semi-sitting position by regulating the functional bed. The patient’s neck and chest is covered with an apron or a napkin. Bedstands are used for feeding the patients; debilitated patients are fed with a spoon. Food is given in small portions, it should be strained and grinded. Special drinking bowls are used for drinking and fluid diet. Patients who cannot chew themselves (in cases of some mouth cavity diseases) or who refuse to eat (in cases of mental diseases) have to be fed through the gastric tube. The tube is introduced through the inferior nasal meatus 15-18 cm deep, then it is slowly moved along the splanchnic wall of the throat while the patient’s head is thrown back. The tube goes to the nasopharynx and then to the gullet along the back of the throat. If the tube goes to the larynx instead of the gullet, the patient has brassy cough and the inhaled and exhaled air goes through the tube. When the tube goes to the gullet, a funnel is put on the free end of the tube. Two or three glasses of different nutrients (broth, cream, milk, fruit jelly, juices) are poured through this funnel. When the fluid diet doesn’t go into the gullet (burns or swelling of the gullet), patients are fed through a specially created stomach fistula. In this case the tube is introduced directly into the stomach.
|
|
Sometimes the patients are fed with the help of nutrient enemas. They are given after the rectum is emptied by a regular enema. After that 5% solution of glucose or 0,85% solution of sodium chloride warmed up to 36-40°С is introduced into the rectum. 100-200 ml. of these solutions are introduced 3-4 times a day. If the patient holds nutrient solutions badly, 5-6 drops of opium extract are added into them.
When patients are seriously ill, nutrient solutions can be administered parenterally, the best way is drip phleboclysis. Usually 40% solution of glucose is used, the blood is transfused, dry blood, plasma substitute, hydrolyzates (hydrolysine, amino peptide, hydrolized protein), which contain all the necessary amino acids, are introduced. 2-3 litres of liquid are introduced a day.
During meals the ward should be clean, the patients should be quiet. If the patient falls asleep, he should be woken. However if the patient was given a narcotic drug or a sleeping pill, he is not to be woken.
To follow all the rules of nutritional care there should be stringent control of food, received for feeding patients in a hospital, and of foodstuffs brought by visitors. Mean medical personnel performs such control. The nurse should have a list of patients with the number of the diet prescribed. In the admission room and in the department of hospital instructions should be posted up stating the amount and kinds of food that patients are allowed to eat. There must be refrigerators in wards for storing food; doctors and nurses are to examine the quality of food in refrigerators and bedside tables regularly.
Body temperature, its taking
and attending febrile patients
Signs of diseases can be specific and non-specific. Temperature rise is a non-specific disease sign. Clinical thermometer was first proposed by Fahrenheit in 1723. At present Celsius mercurial clinical thermometer is used. Clinical thermometer continues to show the maximum temperature which the person had during temperature taking, since mercury cannot go down into the thermometer reservoir by itself without jogging it purposely. This is due to the special device of the clinical thermometer stem which has a narrow spot that prevents the mercury from going back to the reservoir after taking body temperature.
Temperature rise higher than 37°С is called fever, the cause of it is the loop of thermal control which is connected with formation of special substances in the patient’s organism, the so-called pyrogens that change the activity of heat-regulating centres. Most often this happens in cases of infectious diseases.
It should be noted that although fever was already mentioned in the most ancient of the known sources, which state that even the primitives could not help observing that there were “diseases in cases of which the patient’s body became unusually hot and the face skin – red”, even now there is no irrefragable answer to the simple question “What is fever?” (P.N.Veselkin, 1963). However, registration of temperature, analysis of the temperature curve and proper attendance of febrile patients are important medical procedures.
Normal body temperature of a healthy man is constant with small fluctuations in morning and evening hours and it is not higher than 37°С. Such constancy of temperature depends on the processes of heat production and heat emission in the organism. Balance between heat production and heat emission is established and maintained due to thermotaxis – a process in which production and emission of the organism’s heat is regulated(Fig. 12).
|
|
Heat production is mainly a chemical process; its source is the process of oxidation, i.e. combustion of carbohydrates, fats and partly proteins in all cells and tissues of the organism, first of all in skeletal muscles and liver.
Heat emission is mainly a physical process; in quiet state about 80% of the generated body heat is emitted from the body surface, about 20% – due to evaporation of water during respiration and hidrosis, about 1,5% – with urine and feces.
Normally children have a slightly higher temperature than adults, since oxidation processes necessary for the children’s growth are more intensive. Women’s intensity of oxidation processes can vary during the month due to the periodicity of sexual function. This sometimes causes a temperature rise of several tenths of a degree during menstruation.

Рic. 12. Scheme of body temperature regulation (according to K. Cullande, 1976)
Diurnal oscillations of temperature are in direct relation to fluctuations of oxidation processes connected with work or meals. Morning temperature of healthy people is several tenths of a degree lower than the evening one. Indices of temperature depend on the place where it is taken. So, the temperature of oral mucosa, vagina, rectum are 0,2-0,4°С higher than that on an adult’s skin, taken in the axillary creases and inguinal folds. Average body temperature of adults, taken in the axillary creases, is 36,5-37,5°С, children’s average body temperature is 0,5-1°С higher (37-37,5°С) and that of the old people is lower (35,5-36,5°С). Thus, physiological fluctuations of temperature within the norm do net exceed 1°С. Fluctuations of temperature within a day and the whole period are very important. Temperature taking and its observing are important everyday duties of the nurse of any department. The temperature is taken with a clinical thermometer.
Fahrenheit was the first to introduce clinical thermometer in 1723. In our country Celsius thermometer is used. It consists of a glass tube with a thermometer stem, at the end of which there is a reservoir filled with mercury. This tube is attached to the scale, on which there are points from 34 to 42°С. The volume of mercury that fills the reservoir and a small part of the thermometer stem increases if heated. The level of mercury in the stem rises. After the temperature is taken, the mercury in the stem cannot go down on its own, because the pin soldered into the bottom of the reservoir prevents it. The mercury can be brought back only by jogging it several times. This should be done carefully in order not to drop the thermometer or hit it on some closely situated objects. Mercury is very dangerous, if it comes out of the thermometer one should immediately try to collect it wearing gloves and a respirator and report to the doctor or chief of the department. Patients should be evacuated from the room, a special toxicological team should be sent after. Poisoning by mercury vapour can lead to severe consequences right up to death. One must not give a thermometer to children and children are not to be left alone while taking the temperature.
A glass with a layer of cotton-wool on the bottom is usually used for storing thermometers. For 1/3 or Ѕ of the volume the glass is filled with 70% alcohol or Karetnikov’s solution (12 gr. of sodium hydrogencarbonate, 16 gr. of formaline and 3 gr. of phenylic acid for 1 litre of purified water). If these solutions are missing, any disinfectant solution can be used, for example, 0,5% solution of chloramine. Time of exposure must be strictly observed according to order № 408 and government standard 42-21-2-85.
|
|
A rubber cap is put on the upper end of the thermometer to prevent it from falling out of the hand while jogging it.
The Technique of Taking
and Registrating Body Temperature
Taking the temperature
Before taking the temperature it is necessary to wipe the thermometer thoroughly and, having jogged the mercury in the stem to lower than 35 оС, to give it to the patient. The axillary crease is to be wiped with a dry towel beforehand because moisture cools the mercury and the thermometer will show lower temperature. There should not be any cloth between the thermometer and the body. There should not be any hot-water bottles or ice-bags nearby. There should not be any inflammatory processes (skin reddening, intumescence) in the place where the temperature is taken since there can be a local temperature rise. The nurse supports the arm of the debilitated patient. The procedure of taking the temperature should last not less than 10 minutes.
Body temperature of serious and debilitated patients can be taken in the rectum. Contraindications for taking the temperature in this way are: stool retention, diarrhea, rectum diseases. Before introducing the thermometer into the rectum it is to be smeared with vaseline or any grease and then introduced into the rectum for half of its length while the patient lies sidelong. The buttocks are to bear against each other. After each temperature taking in the rectum the thermometer is to be thoroughly washed with warm water and disinfected in alcohol or in any disinfectant in stock. The children’s temperature is taken in the inguinal fold. To do this, the child’s leg is slightly bent in the hip joint so, that the thermometer is in the created skin fold.
Usually the temperature is taken twice a day, in the morning and in the evening – at 7-8 a.m. and at 4-5 p.m. Indications of the thermometer are filled into the temperature form where dots stand for morning and evening temperature.
Main types of fever are:
1. continued fever (febris continua) – the temperature is high for a long time, during the day the difference between the morning and evening temperature is not more than 1оС; it is typical of lung fever and the 2nd stage of abdominal typhoid (fig.13а);
2. remittent fever (febris remitens) – the temperature is high, diurnal oscillations of temperature are more than 1оС (1-2 оС), minimum morning temperature being higher than 37 оС; it is typical of tuberculosis, purulent diseases, bronchopneumonia, 3rd stage of abdominal typhoid (fig.13b);
3. anetus (febris intermittens) – short rises of temperature up to high figures alternate regularly with periods (1-2 days) of normal temperature; may be observed in cases of fever and ague (fig.13c);

Р ic ..13.( а ) Type of continued fever

Р ic ..13.(b) Type of remittent fever

Р ic ..13.(b) Type of intermittens fever
4. intermittent fever (febris undulats) – recurring rises of temperature give place to defervescence down to normal figures. Such “waves” follow each other for a long time. It is typical of Malta fever, lymphogranuloma (fig.14а);
5. recurrent fever (febris recurrens) – regular alternation of high temperature and afebrile periods. Temperature rises and drops very quickly. Febrile and afebrile stages last for several days each. It is typical of bilious typhoid (fig.14b);
6. fever of inverse type (febris inversa) – morning temperature is higher than the evening one; it can sometimes be observed in cases of lues, tuberculosis, Malta fever (fig.14c);
7. abnormal fever (febris irregularis) – is notable for various and irregular diurnal oscillations; it can often be observed in cases of rheumatic disease, endocarditis, sepsis, tuberculosis. This fever is also called atypical (irregular) (fig.14d).

Р ic ..14.(a) Type of undulats fever
During fever several periods are distinguished: period of temperature rising (stadium incrementi), period of high temperature (fastigium), period of temperature dropping (stadium decrementi). Quick drop of high temperature (during several hours) to normal is called crisis, gradual drop of temperature (during several days) is called lysis (fig.15).

Р ic ..14.(b) Type of recurrent fever

Р ic ..14.(c) Fever of inverse type

Р ic ..14.(d) Type of abnormal fever
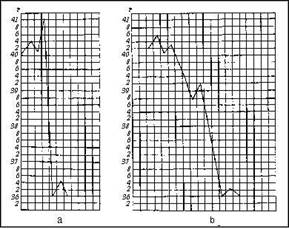
Fig. 15. a - crisis; b - lysis
Sometimes short-term temperature rises can be observed during several hours (ephemeral fever – febris ephemera or febriculara); it occurs in cases of mild infections, sun hyperthermia, after blood transfusion, sometimes after intravenous administration of drugs.
|
|
Fever lasting for less than 15 days is called acute, for over 45 days – chronic.
Most often causes of fever are infectious diseases and formation of tissue decay products (e.g. infarct focus in case of heart attack). Fever is usually the organism’s reaction to infection. Sometimes infectious diseases may not cause fever or may temporarily proceed without temperature rise (tuberculosis, lues, etc.). The level of temperature rise much depends on the patient’s organism: having one and the same disease different people may have different temperature. Thus, in cases of infectious diseases young people with hyperresponsiveness of the organism may run the temperature of 40оС and higher, while older people with suppressed responsiveness do not run temperature at all or have only low-grade fever. The level of temperature rise does not always correspond with the severity of illness but is connected with individual peculiarities of the organism’s responsiveness.
Temperature rise of non-infectious origin is often observed in cases of malignant swellings, necrosis (e.g. infraction), haemorrhage, quick erythrocytoschisis, fallout of alien hypodermic or intravenous substances of albuminous nature. Much rarer fever is observed in cases of central nervous system diseases and diseases of reflex origin. In this case temperature rises are oftener observed in day hours, for which reason it is necessary to take the temperature hourly.
Hypothermia (temperature below the norm – subnormal) is observed in different states: severe circulatory deficiency, profuse blood loss, starvation and cachexia; during recuperation after infectious diseases, in cases of long exposure to cold, crucial temperature drop.
Attending Febrile Patients
In cases of fever all kinds of metabolism are in disorder. The amount of nitrogen coming out with urine increases, there develops hyperglycemia, sometimes – glucosuria, fat metabolism increases, fluid-and-electrolyte balance suffers. Temperature rise by 1оС usually causes acceleration of cardiac rhythm by 10 beats. Breathing rate in cases of fever increases together with acceleration of cardiac beat and temperature rise. Since temperature reflects the level of the organism’s responsiveness, it can be an important index of its status in fight against infection. However it is not always that fever can be regarded as an ausfigious phenomenon, since a very high temperature rise, just like its sudden drop, can be harmful for the organism. In each particular case it is necessary to assess the fever course and its role for the organism.
Fever course is divided into three main periods which the nurse is to know because her actions must differ during each period.
The first period is the period of temperature rise which is accompanied by sudden algor, blue lips, cyanosis of extremities, headaches and overall bad health, when heat production prevails over heat emission. This period lasts from several hours to several days and even weeks. Sudden temperature rise is the most grievous factor for the patient because of strong algor, aches and acute panalgia. During this period the nurse should cover the patient warmly, lay him with hot-water bottles, especially the feet, give him tea with sugar or any other hot drink, watch over all his intestinal habits and there should not be any draughts.
The second period – period of maximum temperature rise – is characterized by aggravation of toxic state, by headache, feeling of fever, dry mouth, sudden asthenia, acute panalgia. During the height of fever the patient may have delirium, hallucinations. Increased heat emission and production are relatively in balance. The period lasts from several hours to several weeks. In cases of fever besides thermotaxis disorders metabolism suffers too. On the one hand combustion augments but on the other, since digestion and absorption slow down, less nutrients are admitted by the organism. This leads to “burning” of the organism’s own tissues, of liver carbohydrates and fatty tissue fats. Proteins are subject to decomposition. The patient becomes debilitated. The higher the temperature, the bigger its swing, the longer it is run, the more the patient is debilitated.
Increase of responsiveness makes it necessary to organize individual post of the nurse or of the junior nurse. If possible, relatives can be admitted to the patient after the nurse has given them a talk about the peculiarities of attending serious patients. Bringing in relatives is impossible in cases of infectious diseases (sequestration). In this case staff schedule of the hospital is reconsidered and persons (hospital attendants) trained in attending serious patients are provided. If during observation the patient’s status becomes worse, it is necessary to inform the duty doctor. During this period the patient should be given high-calorie and easily digestible food in fluid or semiliquid form 5-6 times a day in small portions together with abundant beverage (fruit and berry juices, drinks, mineral water). Patients have dry mouth, labial fissures, that is why it is necessary to wipe their mouths with a dilution of sodium bicarbonate and smear the lips with some oil from time to time. In cases of acute headaches an ice-bag is put on the forehead (it is necessary to change the ice-bag as the ice melts) or a cold compress made of linen cloth or towel folded in four and wetted in vinegar solution (2 table-spoons for 0,5 l of water). The nurse should see to it that it is warm and quiet in the ward, as well as she is to control the patients’ pulse and blood pressure.
The third period is the period of temperature drop. Heat production is usually low and heat emission is high. Quick (during several hours) temperature drop is called crisis, slow (during several days) – lysis. Temperature drop, especially a critical one, is hard for patients because acute cardiovascular collapse often takes place. Quick temperature drop lower than the normal level is accompanied by a sudden change for the worse of the patient’s status. He feels strong asthenia, thirst, cold, algor. Sometimes asthenia is so strong that the patient cannot complain or respond to the surroundings. His skin becomes pale, then blue and covered with cold sweating, his extremities grow cold. Blood pressure suddenly goes down, pulse becomes quick, small (thready pulse), respiration rate increases and breathing becomes shallow. Pupils widen. There develops acute cardiovascular collapse. Crisis may take an ausfigious course when temperature drop is accompanied by abundant sweating, pulse and breathing rate are normal, consciousness is regained, and febrile excitement and insomnia give place to sleep. In case of adverse crisis state the duty nurse or the sick attendant immediately report to the duty doctor about the change for the worse of the patient’s status.
If there is a delay or time-lag in rendering aid, the patient may die because of sudden acute cardiovascular collapse. Duty doctor assess the patient’s status, renders first aid, gives prescriptions that are to be immediately fulfilled by the duty nurse. As a rule drugs that rise blood pressure (Mesaton, caffeine, epinephrine) are administered hypodermically. The patient is laid with hot-water bottles, given strong warm tea or coffee, his underclothes and, if necessary, bed linen is changed. Critical temperature drop can be observed in cases of lung fever, a number of infectious diseases.
Gradual temperature drop is called lytic. It is accompanied by slight perspiration on skin and asthenia. After temperature drop the patient usually falls asleep. Sleep is the best remedy.
If the patient has been febrile for a long time, the nurse should see to the toilet of skin integument, which is carried out by the junior nurse. If there is no junior nurse in the staff schedule, these duties must be performed by the duty nurse. Bedsore prevention is the most important among the duties. Besides temperature the following indices are recorded in temperature forms: pulse, blood pressure, respiration rate, weight, amount of drunk and discharged liquid, kind of stool. Febrile patients must discharge all intestinal habits in bed (the patient is given a bedpan). In case of constipation a cleansing enema is given. It must be mentioned that high enema (and not laxatives) can lower body temperature and thus improve the patient’s status.
 Рис. 16. Приготовление резиновой грелки
Водолечебные процедуры (бальнеотерапия)
ванны, обливания, обтирания, влажные обертывания, душ.
Холодная (до 20 оС) и прохладная (20—ЗО оС) вода вызывает спазм сосудов кожи, замедление ЧСС, повышение АД тонуса скелетных мышц, гладкой мускулатуры внутренних органов; применяется с общеукрепляющей и закаливающей целями, для стимуляции функции ЦНС, повышения обмена веществ. Индифферентная вода (34—36°С) оказывает заметный седативный, расслабляющий эффект. Теплая (37—39°С) и горячая (свыше 40 оС) вода производит отчетливое возбуждающее действие, расширение сосудов кожи, учащение ЧСС, снижение АД и мышечного тонуса, расслабление гладкой мускулатуры внутренних органов, усиление потоотделения.
Ванны бывают гигиеническими и лечебными, общими и местными. В зависимости от состава воды выделяются жемчужные (пузырьки воздуха под давлением), пенистые (пенообразующие вещества), вибрационные и вихревые (усиление механического фактора воды), ароматические (хвойные, шалфейные и т.д.), минеральные (сероводородные) и другие ванны. По продолжительности они бывают кратковременные (до 5 мин.), средней продолжительности (10—20 мин.), длительные (до нескольких часов).
Противопоказания: тяжелый атеросклероз, гипертоническая болезнь, недостаточность кровообращения, нарушение мозгового и коронарного кровообращения, активный туберкулез.
При применении лечебных ванн и других водных процедур необходимо тщательно следить за состоянием больных, которое из-за изменения АД, ЧСС и дыхания может иногда внезапно ухудшиться
Пути введения лекарственных веществ в организм
Наружное применение лекарств
1. На кожу наносят лекарства в форме мазей, эмульсий, растворов, настоек, болтушек и т. д. Применение рассчитано в основном на местное действие, на выраженный в значительной степени рефлекторный и небольшой степени резорбтивный эффекты. Всасывающая способность неповрежденной кожи весьма незначительна, всасываются только жирорастворимые вещества, причем главным образом через выводные протоки сальных желез и волосяных фолликулов.
Способы применения: смазывания, компрессы, примочки, присыпки, различные повязки на раны и втирания. Нанесение лекарств должно производиться всегда на чистую кожу, чистыми инструментами и тщательно вымытыми руками.
С целью дезинфекции или для оказания рефлекторного воздействия кожу смазывают настойкой йода или 70% раствором спирта. Для этого берут стерильную палочку с ватным тампоном, смачивают йодом и смазывают кожу (затем палочку выбрасывают). Смачивая вату, нельзя погружать палочку во флакон с йодом, следует отлить небольшое количество настойки йода в плоский сосуд, чтобы не загрязнить все содержимое флакона хлопьями ваты.
При длительном хранении настойки йода в посуде с неплотно пригнанной пробкой концентрация ее может повышаться за счет испарения спирта. Смазывание концентрированной настойкой йода нежных участков кожи может вызвать ожог.
2. При лечении глазных заболеваний применяют растворы различных лекарственных веществ и мази.
Цель применения — местное воздействие, но следует помнить о хорошей всасывающей способности конъюнктивы и дозировать лекарства с учетом этой возможности.
Закапывание лекарства в глаз производят пипеткой. Для этого оттягивают нижнее веко и наносят каплю на слизистую оболочку ближе к наружному углу глаза, чтобы раствор равномерно распределился по конъюнктиве. Глазную мазь специальной стеклянной лопаточкой вносят в щель между слизистой оболочкой конъюнктивы и глазным яблоком у наружного угла глаза.
3. В нос применяют лекарства в виде порошков, паров (амилнитрат, пары нашатырного спирта), растворов и мазей с целью местного, резорбтивного и рефлекторного воздействий. Всасывание через слизистую оболочку носа происходит очень энергично.
Порошки втягиваются в нос струей вдыхаемого воздуха: закрыв правую ноздрю, порошок вдыхают через левую и наоборот. Капли вводят пипеткой, при этом больной запрокидывает голову назад. Мазь вносят стеклянной лопаточкой. Смазывание производит врач ватным тампоном, накрученным на зонд, после этого тампон выбрасывают, а зонд стерилизуют в дезрастворе.
4. В уши лекарства закапывают также пипеткой. Масляные растворы лекарственных веществ следует подогревать до температуры тела. При закапывании в правый наружный слуховой проход больной ложится на левый бок или наклоняет голову влево и наоборот. После введения лекарства наружный слуховой проход закрывают ватным тампоном.
5. Для воздействия на женские половые органы лекарства во влагалище вводят в виде шариков, сделанных на масле какао, ватно-марлевых тампонов, пропитанных различными жидкостями и маслами, порошков (присыпки), растворов для смазывания и спринцеваний. Действие медикаментов в основном местное, так как через неповрежденную слизистую оболочку влагалища всасывание незначительно. Спринцевание производят при помощи кружки Эсмарха со специальным влагалищным наконечником или резиновой груши, под таз больного при этом подкладывают судно. Для спринцевания используют теплые растворы лекарств или настои лекарственных трав по назначению врача.
Энтеральное введение лекарств
Внутрь лекарство вводят через рот (per os), прямую кишку (per rectum) и под язык (sub lingua). С помощью всех этих способов можно получить местное, резорбтивное и рефлекторное действия.
I. Введением лекарств через рот (per os) пользуются чаще всего. Достоинства этого способа заключаются в простоте, возможности вводить лекарства в самых различных формах и в нестерильном виде. К числу его недостатков относятся:
1. Медленное поступление лекарства в общий круг кровообращения (в зависимости от наполнения желудка, качества наполняющей пищи, способностей медикамента к всасыванию). Всасывание через слизистую оболочку желудка происходит также медленно, причем всасываются только жирорастворимые вещества, и процесс всасывания в основном происходит в кишечнике. Но медленное поступление лекарственного вещества в кровоток не всегда является недостатком. Так, существуют лекарственные формы, специально разработанные для длительного, равномерного поступления вещества в общий круг кровообращения после однократного приема внутрь.
2. Изменение лекарства вплоть до разрушения под влиянием желудочного и кишечного соков, в результате взаимодействия с пищевыми веществами (абсорбция, растворение, химические реакции) и химических превращений в печени. Это справедливо не для всех медикаментов. Так, некоторые лекарственные вещества изначально выпускают в виде неактивной субстанции, которая становится действующим веществом только после превращения в печени. Например, гипотензивный препарат эналаприл (ренитек) прежде чем оказать свое действие должен преобразоваться в печени в свою активную форму (эналаприлат).
3. Невозможность предусмотреть создающуюся концентрацию лекарства в крови и в тканях из-за неопределенной скорости всасывания и количества всасывающегося вещества. Чтобы уменьшить эти отрицательные влияния, лекарства применяют перед едой (за исключением лекарств, раздражающих слизистую оболочку желудка), защищают их от воздействия желудочного сока, помещая в капсулы, вводят в двенадцатиперстную кишку через зонд.
Заболевания желудочно-кишечного тракта и печени вносят особые трудно учитываемые изменения в скорость и полноту всасывания лекарственных средств.
Через рот вводят лекарства в форме порошков, таблеток, пилюль, растворов, настоев (водных и спиртовых), отваров, экстрактов, микстур (смесей).
Порошок медсестра высыпает больному на корень языка и дает запить водой. Так же больной принимает таблетку и пилюлю. Дети не всегда могут принять порошок или таблетку, поэтому последние разводят в воде и дают им выпить взвесь.
Растворы, водные настои и микстуру взрослые получают по столовой ложке (15 г), дети — по чайной (5 г) или десертной ложке (7,5 г). Рекомендуется для этой цели пользоваться мензуркой с соответствующими делениями. Жидкие лекарства неприятного вкуса запивают водой.
Спиртовые настойки и некоторые растворы больные получают в виде капель. Нужное количество капель следует отсчитывать пипеткой или прямо из флакона, если флакон имеет специальное для этого приспособление. Перед приемом капли растворяют небольшим количеством воды и запивают водой. Если произошла ошибка в счете капель, лекарство нужно вылить (не во флакон), ополоснуть мензурку и вновь накапать нужное число капель. Для расчетов следует знать, что в 1 г воды содержится 20 капель, в 1г. спирта — 65 капель, эфира — 85 капель.
II. Введение лекарств через прямую кишку (per rectum) имеет следующие преимущества:
1. быстрое всасывание и большая точность дозировки;
2. лекарство не подвергается влиянию ферментов, так как их в прямой кишке нет, и, всасываясь, попадает через нижние геморроидальные вены непосредственно в нижнюю полую вену, минуя печень;
3. этот способ дает возможность дать лекарство тем больным, которые не могут принять его через рот из-за рвоты, непроходимости пищевода, нарушения акта глотания (в том числе больным, находящимся в бессознательном состоянии), психическим больным, отказывающимся принимать лекарство, при возбуждении (бредовом состоянии), когда прием лекарств через рот невозможен, а впрыскивание трудно выполнимо и сопряжено с опасностью. В этих случаях введение успокаивающих средств с лекарственной клизмой (например раствор хлоргидрата) дает возможность успешно бороться с возбуждением.
Отсутствие ферментов в прямой кишке обусловливает не только достоинство, но и недостаток этого способа введения, так как лекарства белковой, жировой и полисахаридной структуры не могут пройти через кишечную стенку без участия ферментов, и применение их возможно только с целью местного воздействия.
Для введения в прямую кишку пользуются свечами и лекарственными клизмами. Раствор лекарства в количестве 50—200 мл вводят в прямую кишку, предварительно освобожденную очистительной клизмой, на глубину 7—8 см. Свечи приготавливают на жировой основе, придают им форму удлиненного конуса и заворачивают в вощеную бумагу. Хранить их лучше в холодильнике. Перед введением заостренный конец свечи освобождают от бумаги и вводят в прямую кишку так, чтобы обертка осталась в руке.
III. При введении под язык лекарство быстро всасывается, не разрушается пищеварительными ферментами и поступает в общий ток кровообращения, минуя печень. Однако этим способом можно пользоваться только для введения лекарств, применяемых в небольших дозах (так принимают нитроглицерин, некоторые гормоны и др.).
Введение лекарств в дыхательные пути
При различных заболеваниях дыхательных путей и легких пользуются введением лекарств непосредственно в дыхательные пути. Чаще лекарственное вещество вводят в форме аэрозоля путем его вдыхания — ингаляции, реже раствор лекарства вливают в трахею через резиновую трубочку или через трубку специального прибора — бронхоскопа. Интратрахеальное введение пенициллина дает хорошие результаты при лечении острого и хронического абсцесса (гнойника) легкого.
При введении лекарств в дыхательные пути можно получить местный, резорбтивный и рефлекторный эффекты.
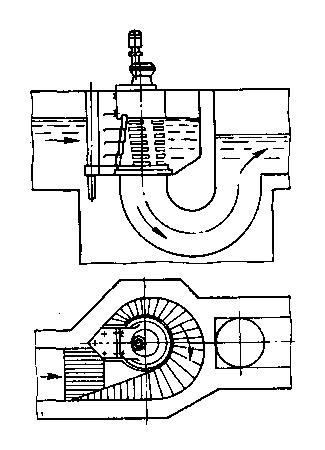
При лечении больных с катаром верхних дыхательных путей и ангиной издавна пользуются паровой ингаляцией при помощи простейшего ингалятора. Струя пара, образующегося в водяном подогреваемом бачке, выбрасывается по горизонтальной трубке распылителя и разрежает воздух под вертикальным коленом, вследствие этого лекарственный раствор из стаканчика поднимается по вертикальной трубке и разбивается паром на мельчайшие частицы. Пар с частицами лекарства попадает в стеклянную трубку, которую больной берет в рот и дышит (делая вдох ртом, а выдох носом) 5-10 минут. В домашних условиях вместо ингалятора можно использовать чайник, в носик которого вставляют бумажную или пластмассовую трубку, вдыхание проводится ч
Рис. 16. Приготовление резиновой грелки
Водолечебные процедуры (бальнеотерапия)
ванны, обливания, обтирания, влажные обертывания, душ.
Холодная (до 20 оС) и прохладная (20—ЗО оС) вода вызывает спазм сосудов кожи, замедление ЧСС, повышение АД тонуса скелетных мышц, гладкой мускулатуры внутренних органов; применяется с общеукрепляющей и закаливающей целями, для стимуляции функции ЦНС, повышения обмена веществ. Индифферентная вода (34—36°С) оказывает заметный седативный, расслабляющий эффект. Теплая (37—39°С) и горячая (свыше 40 оС) вода производит отчетливое возбуждающее действие, расширение сосудов кожи, учащение ЧСС, снижение АД и мышечного тонуса, расслабление гладкой мускулатуры внутренних органов, усиление потоотделения.
Ванны бывают гигиеническими и лечебными, общими и местными. В зависимости от состава воды выделяются жемчужные (пузырьки воздуха под давлением), пенистые (пенообразующие вещества), вибрационные и вихревые (усиление механического фактора воды), ароматические (хвойные, шалфейные и т.д.), минеральные (сероводородные) и другие ванны. По продолжительности они бывают кратковременные (до 5 мин.), средней продолжительности (10—20 мин.), длительные (до нескольких часов).
Противопоказания: тяжелый атеросклероз, гипертоническая болезнь, недостаточность кровообращения, нарушение мозгового и коронарного кровообращения, активный туберкулез.
При применении лечебных ванн и других водных процедур необходимо тщательно следить за состоянием больных, которое из-за изменения АД, ЧСС и дыхания может иногда внезапно ухудшиться
Пути введения лекарственных веществ в организм
Наружное применение лекарств
1. На кожу наносят лекарства в форме мазей, эмульсий, растворов, настоек, болтушек и т. д. Применение рассчитано в основном на местное действие, на выраженный в значительной степени рефлекторный и небольшой степени резорбтивный эффекты. Всасывающая способность неповрежденной кожи весьма незначительна, всасываются только жирорастворимые вещества, причем главным образом через выводные протоки сальных желез и волосяных фолликулов.
Способы применения: смазывания, компрессы, примочки, присыпки, различные повязки на раны и втирания. Нанесение лекарств должно производиться всегда на чистую кожу, чистыми инструментами и тщательно вымытыми руками.
С целью дезинфекции или для оказания рефлекторного воздействия кожу смазывают настойкой йода или 70% раствором спирта. Для этого берут стерильную палочку с ватным тампоном, смачивают йодом и смазывают кожу (затем палочку выбрасывают). Смачивая вату, нельзя погружать палочку во флакон с йодом, следует отлить небольшое количество настойки йода в плоский сосуд, чтобы не загрязнить все содержимое флакона хлопьями ваты.
При длительном хранении настойки йода в посуде с неплотно пригнанной пробкой концентрация ее может повышаться за счет испарения спирта. Смазывание концентрированной настойкой йода нежных участков кожи может вызвать ожог.
2. При лечении глазных заболеваний применяют растворы различных лекарственных веществ и мази.
Цель применения — местное воздействие, но следует помнить о хорошей всасывающей способности конъюнктивы и дозировать лекарства с учетом этой возможности.
Закапывание лекарства в глаз производят пипеткой. Для этого оттягивают нижнее веко и наносят каплю на слизистую оболочку ближе к наружному углу глаза, чтобы раствор равномерно распределился по конъюнктиве. Глазную мазь специальной стеклянной лопаточкой вносят в щель между слизистой оболочкой конъюнктивы и глазным яблоком у наружного угла глаза.
3. В нос применяют лекарства в виде порошков, паров (амилнитрат, пары нашатырного спирта), растворов и мазей с целью местного, резорбтивного и рефлекторного воздействий. Всасывание через слизистую оболочку носа происходит очень энергично.
Порошки втягиваются в нос струей вдыхаемого воздуха: закрыв правую ноздрю, порошок вдыхают через левую и наоборот. Капли вводят пипеткой, при этом больной запрокидывает голову назад. Мазь вносят стеклянной лопаточкой. Смазывание производит врач ватным тампоном, накрученным на зонд, после этого тампон выбрасывают, а зонд стерилизуют в дезрастворе.
4. В уши лекарства закапывают также пипеткой. Масляные растворы лекарственных веществ следует подогревать до температуры тела. При закапывании в правый наружный слуховой проход больной ложится на левый бок или наклоняет голову влево и наоборот. После введения лекарства наружный слуховой проход закрывают ватным тампоном.
5. Для воздействия на женские половые органы лекарства во влагалище вводят в виде шариков, сделанных на масле какао, ватно-марлевых тампонов, пропитанных различными жидкостями и маслами, порошков (присыпки), растворов для смазывания и спринцеваний. Действие медикаментов в основном местное, так как через неповрежденную слизистую оболочку влагалища всасывание незначительно. Спринцевание производят при помощи кружки Эсмарха со специальным влагалищным наконечником или резиновой груши, под таз больного при этом подкладывают судно. Для спринцевания используют теплые растворы лекарств или настои лекарственных трав по назначению врача.
Энтеральное введение лекарств
Внутрь лекарство вводят через рот (per os), прямую кишку (per rectum) и под язык (sub lingua). С помощью всех этих способов можно получить местное, резорбтивное и рефлекторное действия.
I. Введением лекарств через рот (per os) пользуются чаще всего. Достоинства этого способа заключаются в простоте, возможности вводить лекарства в самых различных формах и в нестерильном виде. К числу его недостатков относятся:
1. Медленное поступление лекарства в общий круг кровообращения (в зависимости от наполнения желудка, качества наполняющей пищи, способностей медикамента к всасыванию). Всасывание через слизистую оболочку желудка происходит также медленно, причем всасываются только жирорастворимые вещества, и процесс всасывания в основном происходит в кишечнике. Но медленное поступление лекарственного вещества в кровоток не всегда является недостатком. Так, существуют лекарственные формы, специально разработанные для длительного, равномерного поступления вещества в общий круг кровообращения после однократного приема внутрь.
2. Изменение лекарства вплоть до разрушения под влиянием желудочного и кишечного соков, в результате взаимодействия с пищевыми веществами (абсорбция, растворение, химические реакции) и химических превращений в печени. Это справедливо не для всех медикаментов. Так, некоторые лекарственные вещества изначально выпускают в виде неактивной субстанции, которая становится действующим веществом только после превращения в печени. Например, гипотензивный препарат эналаприл (ренитек) прежде чем оказать свое действие должен преобразоваться в печени в свою активную форму (эналаприлат).
3. Невозможность предусмотреть создающуюся концентрацию лекарства в крови и в тканях из-за неопределенной скорости всасывания и количества всасывающегося вещества. Чтобы уменьшить эти отрицательные влияния, лекарства применяют перед едой (за исключением лекарств, раздражающих слизистую оболочку желудка), защищают их от воздействия желудочного сока, помещая в капсулы, вводят в двенадцатиперстную кишку через зонд.
Заболевания желудочно-кишечного тракта и печени вносят особые трудно учитываемые изменения в скорость и полноту всасывания лекарственных средств.
Через рот вводят лекарства в форме порошков, таблеток, пилюль, растворов, настоев (водных и спиртовых), отваров, экстрактов, микстур (смесей).
Порошок медсестра высыпает больному на корень языка и дает запить водой. Так же больной принимает таблетку и пилюлю. Дети не всегда могут принять порошок или таблетку, поэтому последние разводят в воде и дают им выпить взвесь.
Растворы, водные настои и микстуру взрослые получают по столовой ложке (15 г), дети — по чайной (5 г) или десертной ложке (7,5 г). Рекомендуется для этой цели пользоваться мензуркой с соответствующими делениями. Жидкие лекарства неприятного вкуса запивают водой.
Спиртовые настойки и некоторые растворы больные получают в виде капель. Нужное количество капель следует отсчитывать пипеткой или прямо из флакона, если флакон имеет специальное для этого приспособление. Перед приемом капли растворяют небольшим количеством воды и запивают водой. Если произошла ошибка в счете капель, лекарство нужно вылить (не во флакон), ополоснуть мензурку и вновь накапать нужное число капель. Для расчетов следует знать, что в 1 г воды содержится 20 капель, в 1г. спирта — 65 капель, эфира — 85 капель.
II. Введение лекарств через прямую кишку (per rectum) имеет следующие преимущества:
1. быстрое всасывание и большая точность дозировки;
2. лекарство не подвергается влиянию ферментов, так как их в прямой кишке нет, и, всасываясь, попадает через нижние геморроидальные вены непосредственно в нижнюю полую вену, минуя печень;
3. этот способ дает возможность дать лекарство тем больным, которые не могут принять его через рот из-за рвоты, непроходимости пищевода, нарушения акта глотания (в том числе больным, находящимся в бессознательном состоянии), психическим больным, отказывающимся принимать лекарство, при возбуждении (бредовом состоянии), когда прием лекарств через рот невозможен, а впрыскивание трудно выполнимо и сопряжено с опасностью. В этих случаях введение успокаивающих средств с лекарственной клизмой (например раствор хлоргидрата) дает возможность успешно бороться с возбуждением.
Отсутствие ферментов в прямой кишке обусловливает не только достоинство, но и недостаток этого способа введения, так как лекарства белковой, жировой и полисахаридной структуры не могут пройти через кишечную стенку без участия ферментов, и применение их возможно только с целью местного воздействия.
Для введения в прямую кишку пользуются свечами и лекарственными клизмами. Раствор лекарства в количестве 50—200 мл вводят в прямую кишку, предварительно освобожденную очистительной клизмой, на глубину 7—8 см. Свечи приготавливают на жировой основе, придают им форму удлиненного конуса и заворачивают в вощеную бумагу. Хранить их лучше в холодильнике. Перед введением заостренный конец свечи освобождают от бумаги и вводят в прямую кишку так, чтобы обертка осталась в руке.
III. При введении под язык лекарство быстро всасывается, не разрушается пищеварительными ферментами и поступает в общий ток кровообращения, минуя печень. Однако этим способом можно пользоваться только для введения лекарств, применяемых в небольших дозах (так принимают нитроглицерин, некоторые гормоны и др.).
Введение лекарств в дыхательные пути
При различных заболеваниях дыхательных путей и легких пользуются введением лекарств непосредственно в дыхательные пути. Чаще лекарственное вещество вводят в форме аэрозоля путем его вдыхания — ингаляции, реже раствор лекарства вливают в трахею через резиновую трубочку или через трубку специального прибора — бронхоскопа. Интратрахеальное введение пенициллина дает хорошие результаты при лечении острого и хронического абсцесса (гнойника) легкого.
При введении лекарств в дыхательные пути можно получить местный, резорбтивный и рефлекторный эффекты.
При лечении больных с катаром верхних дыхательных путей и ангиной издавна пользуются паровой ингаляцией при помощи простейшего ингалятора. Струя пара, образующегося в водяном подогреваемом бачке, выбрасывается по горизонтальной трубке распылителя и разрежает воздух под вертикальным коленом, вследствие этого лекарственный раствор из стаканчика поднимается по вертикальной трубке и разбивается паром на мельчайшие частицы. Пар с частицами лекарства попадает в стеклянную трубку, которую больной берет в рот и дышит (делая вдох ртом, а выдох носом) 5-10 минут. В домашних условиях вместо ингалятора можно использовать чайник, в носик которого вставляют бумажную или пластмассовую трубку, вдыхание проводится ч|
|
|
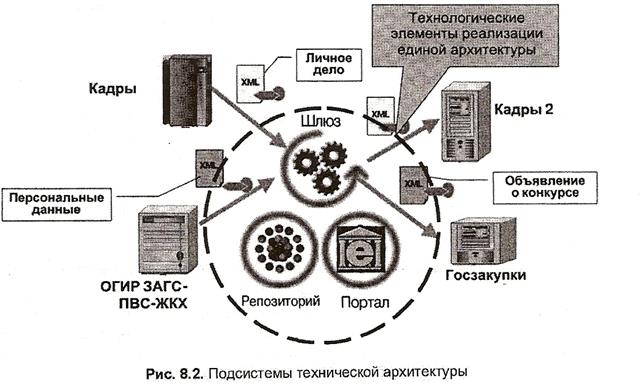
Архитектура электронного правительства: Единая архитектура – это методологический подход при создании системы управления государства, который строится...
Папиллярные узоры пальцев рук - маркер спортивных способностей: дерматоглифические признаки формируются на 3-5 месяце беременности, не изменяются в течение жизни...
Семя – орган полового размножения и расселения растений: наружи у семян имеется плотный покров – кожура...
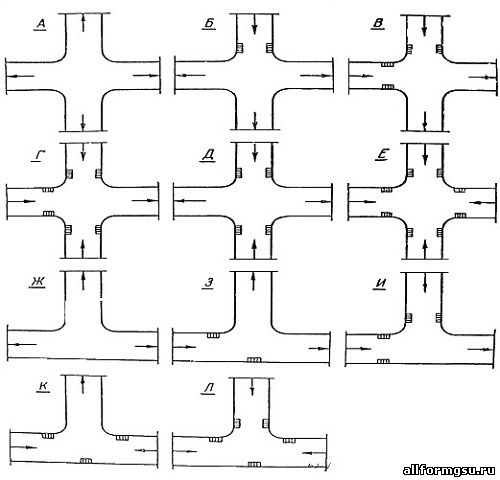
Организация стока поверхностных вод: Наибольшее количество влаги на земном шаре испаряется с поверхности морей и океанов (88‰)...
© cyberpedia.su 2017-2024 - Не является автором материалов. Исключительное право сохранено за автором текста.
Если вы не хотите, чтобы данный материал был у нас на сайте, перейдите по ссылке: Нарушение авторских прав. Мы поможем в написании вашей работы!