
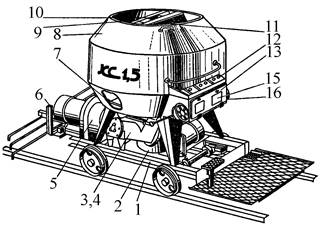
Кормораздатчик мобильный электрифицированный: схема и процесс работы устройства...
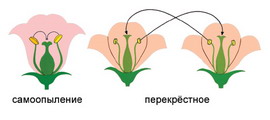
Семя – орган полового размножения и расселения растений: наружи у семян имеется плотный покров – кожура...
Кормораздатчик мобильный электрифицированный: схема и процесс работы устройства...
Семя – орган полового размножения и расселения растений: наружи у семян имеется плотный покров – кожура...
Топ:
Методика измерений сопротивления растеканию тока анодного заземления: Анодный заземлитель (анод) – проводник, погруженный в электролитическую среду (грунт, раствор электролита) и подключенный к положительному...
Процедура выполнения команд. Рабочий цикл процессора: Функционирование процессора в основном состоит из повторяющихся рабочих циклов, каждый из которых соответствует...
Организация стока поверхностных вод: Наибольшее количество влаги на земном шаре испаряется с поверхности морей и океанов...
Интересное:
Распространение рака на другие отдаленные от желудка органы: Характерных симптомов рака желудка не существует. Выраженные симптомы появляются, когда опухоль...
Мероприятия для защиты от морозного пучения грунтов: Инженерная защита от морозного (криогенного) пучения грунтов необходима для легких малоэтажных зданий и других сооружений...
Лечение прогрессирующих форм рака: Одним из наиболее важных достижений экспериментальной химиотерапии опухолей, начатой в 60-х и реализованной в 70-х годах, является...
Дисциплины:
|
из
5.00
|
Заказать работу |
|
|
|
|
Compose a Case Report relying on the data given about the disease. Some information should be added:
1) Cause: Unknown.
Symptoms: Weak pulse, pale face, periodical heart pains, death anxiety, breathlessness. The patient absolutely cannot lie down.
Diagnosis: Heart failure.
Treatment: The patient must be propped up to allow him to breathe or he may be allowed to sit straight up. A cup of coffee or tea may do some good, and will surely do no harm. The patient should be covered to keep him warm. Reassure the patient and give him cardiacs.
2) Cause: Not clear.
Symptoms: The onset is sudden. The pain in the right iliac region and all over the abdomen is acute. The patient feels constant nausea and has profuse vomiting. The temperature is elevated.
Diagnosis: An acute attack of appendicitis.
Treatment: Urgent surgical intervention is necessary. Local anesthesia is indicated. Opening the abdominal cavity with an oblique incision in the right iliac region is to be applied.
3) Cause: A fish bone in the pharynx because of too rapid eating.
Symptoms: The patient feels stinging pain, especially when swallowing.
Diagnosis: A foreign body in the pharynx.
Treatment: An attempt to remove the bone with finger was successfully followed by the extraction of the bone with forceps.
IX.Medical Record
Read the dialogue between Doctor Johnson and a medical student through. Then read and translate the first case below. Using the sections of the medical record Dr. Johnson is reading in the dialogue as a model, fill in the similar sections for Case 1. Continue making up medical records with the same sections for the other cases described.
The diagnoses of these cases are given after the 7th Case. You are not qualified enough yet to find the correct diagnosis to each case. However, you could try, think and guess, relying on some medical knowledge you do have. Prepare to give your reasons why you have chosen the particular diagnosis. Your lecturer will give you the correct diagnosis of the doctors.
Dr.Johnson: So, what is the history of your new case? Let me see it!
Medical Student: Here you are!
Dr.Johnson (reads):
Patient: Paul Brown.
Age: 58.
Sex: Male.
Occupation: Engineer.
Family status: Married.
Family history: Wife and four children living and well; father living and well; mother died: the result of a street accident; two sisters and а brother living and well.
Past history: Measles, scarlet fever and pneumonia in childhood; two ribs fractured: the result of a war wound; neither drinks nor smokes.
Present complaints: A severe pain in the abdomen (the right iliac region); nausea and vomiting; temperature 39ºC.
Duration: 2 days.
Diagnosis: Acute appendicitis.
Dr.Johnson: In most cases, appendicitis is not difficult to diagnose, but sometimes the picture is that of acute intestinal process, e.g. enterocolitis. It is particularly easy to overlook it in children, in whom its course is a violent one and often produces general phenomena with negligible local ones. Children cannot point out the location of pain and often complain of it in the epigastrium or all over the abdomen. Tell me, please, what does his physical examination reveal?
|
|
Medical Student: The physical examination of my patient reveals pain and limited muscular tension in the right iliac region. The clinical picture is the one of acute appendicitis.
Dr.Johnson: I agree with you that his symptoms are those of acute appendicitis.
VOCABULARY OF MEDICAL TERMS TO THE CASE REPORTS:
productive cough влажный кашель
sputum=phlegm мокрота
on exertion=on effort при напряжении
cyanotic blush цианотический румянец
heart sound сердечный тон
clapping sound хлопающий тон сердца
dull sound притупленный, глухой тон
presystolic murmur пресистолический шум
pleural fremitus =rub шум трения плевры
exposure to cold пребывание на холоде
expose to cold подвергать воздействию холода
pulse of an average fullness пульс среднего наполнения
regular shape правильная форма
it is somewhat retarded она несколько отстает
harsh breathing (respiration) жесткое дыхание
amphoric breathing амфорическое дыхание
tympanitic resonance тимпанический звук
loss of resonance притупление перкуторного звука
infiltrate darkening инфильтративное затемнение
erythrocyte sedimentation rate (ESR) СОЭ (скорость оседания эритроцитов)
shift to the left сдвиг влево
vocal fremitus голосовое дрожание
forced position вынужденное положение
injected veins набухшие вены
the border is moved down граница опущена
mobility подвижность
disseminated rales рассеянные хрипы
moist rales влажные хрипы
sonorous coarse rales звучные крупные хрипы
medium bubbling rales средне-пузырчатые хрипы
single rales единичные хрипы
median line средняя линия
from the medioclavicular line out снаружи от средне-ключичной линии
fall into layers распадаться на слои
accent акцент
accentuated акцентуированный
interscapular space межлопаточное пространство
dyspnea одышка
compressing pain сжимающая боль
edema отек
hypochondrium подреберье
vascular wall сосудистая стенка
outside the pulse wave вне пульсовой волны
spread heart beat разлитой сердечный толчок
CASE 1
The doctor was called in as the patient, Eric Someson, complained of high temperature, pains in the right side on deep respiration, dry cough. The onset was sudden, the day before while working he felt malaise, chill, a slight cough appeared. In the evening the temperature was 38ºC, today in the morning it was 38,4ºC. He had never had anything like this illness before. He had suffered from measles, quinsies, now and again an upper respiratory infection. The patient is 38, male, works as a driver. He believes his illness is due to his exposure to cold.
|
|
Objective findings: there is feverish blush on his face, his position is active. The pulse rate is 90 per minute, rhythmic, of an average fullness and tension. His heart borders and sounds are normal. The shape of his chest is regular, the right side of it is somewhat retarded in breathing, respiration rate is 18 per minute. On percussion a dull sound (loss of resonance) was revealed in the right subscapular area. There is slightly harsh breathing and pleural rub in the same area.
CASE 2
Mike Green was brought to the in-patient department as an emergency case with complaints of fever, the temperature being up to 38,5-39ºC, pains in the left side of the chest, especially bad on respiration, cough with a small amount of mucopurulent sputum without any smell. The patient had been ill for a week. The onset had been sudden, the temperature rising to 38ºC, with cough and pains in the left side. He had been on a business trip at the time, and because of this he hadn’t consulted a doctor. Having returned home he called in the doctor who insisted on hospitalization.
The patient is 41, male, works as an engineer at a plant. He believes the cause of his illness to be his exposure to cold. He had hardly any complaints in the past, only once in a while he had an upper respiratory infection or quinsy.
Objective findings: the patient’s general condition is bad, there is feverish blush, dyspnea, superficial breathing, respiration rate is 24 per minute. The pulse rate is 120 per minute, it is small, soft. Blood pressure is 100 over 60 mm. The heart borders are normal, the first sound is slightly dull. The chest on the left is retarded on respiration. On the left at the back the lung border cannot be determined, on the right the lung border is normal. There is a pleural friction rub along the lower side. The vocal fremitus and bronchophony are increased.
CASE 3
Evan Wilson, aged 50, male, was brought to the in-patient department as a case of emergency. He complained of a pain in the right side of his chest which set in abruptly and of short breath. He had been ill with an upper respiratory infection for some days when an acute pain in his side and breathlessness developed on a bad attack of coughing. The temperature is normal. The patient used to suffer from bronchitis in the past, he smokes.
Objective findings: the patient’s general condition is of an average severity, he takes a forced sitting position, respiration rate is 28 per minute, he is pale, his lips are cyanotic, the veins on his neck are injected, the right side of his chest doesn’t take part in the respiration. The breathing is absent over the right side of the chest, over the left side dry rales are heard. Pulse rate is 90 per minute.
CASE 4
The patient, Peter Smith, aged 38, male, has been staying in the in-patient department for 3 weeks. At present he complains of subfebrile temperature, cough with a large amount of sputum (200 gr per day), having a foul smell (if kept it falls into layers), mild pains in the right side of his chest. He had felt ill for a month before, when subfebrile temperature, dry cough and cold in the head appeared. The patient continued working for a week, but then his temperature rose up to 38-39ºC and he was hospitalized. A week ago expectoration of a large amount of purulent sputum developed, his temperature dropped and became subfebrile, his condition somewhat improved.
The patient works as a shopmaster at a factory, he is often exposed to draughts at his shop and frequently catches cold, he had pneumonia twice. He smokes, drinks alcohol regularly, almost daily. He believes his illness is due to his having been exposed to severe cold when drunk.
Objective findings: general condition of the patient is rather severe. The position is active, but he tends to lie on the right side as cough worries him less in this position. The patient is grayish-pale, his pulse is frequent, pulse rate is 90 per minute, heart borders are within the normal limits, the first heart sound is somewhat weakened, the second one is accentuated on the pulmonary artery.
|
|
CASE 5
Jane Melton is 55, female, she was admitted to the in-patient department with the complaints of subfebrile temperature, persistent cough with a small amount of mucopurulent sputum without any smell, a bad general weakness, sweating, a feeling of heaviness and pains in the right side of her chest, especially on deep respiration. She fell ill two weeks ago when cold in the head and malaise appeared. Her temperature was normal, so she continued working. A week later her cough increased, a small amount of sputum appeared, the temperature began to rise. Then the patient was given a sick leave and treated by an expectorating mixture, mustard plasters, aspirin. As her condition didn’t improve, the doctor referred her to the hospital.
Objective findings: the patient’s general condition is not bad, there is no dyspnea. Her pulse is rhythmic, of an average fullness and tension, pulse rate is 86 per minute. Heart borders and sounds are within the normal limits. The chest mobility is normal, there is no retardation in breathing. On percussion the lung borders were found to be normal, on the right there was noticed limited mobility of the lung border along the back surface, loss of resonance in the right intrascapular space, one could hear harsh breathing and fine bubbling moist rales, sonorous ones.
CASE 6
Catherine Reice, aged 30, female, complains of breathlessness, productive cough with expectoration of a small amount of sputum, occasionally bloody. When a child, she used to suffer from quinsies. She had tonsillectomy at 12. Dyspnea first developed two years ago. Breathlessness increased and expectoration of bloody sputum appeared a few days ago on physical exertion.
Objective findings: she has cyanotic blush on her cheeks, her pulse rate is 120 per minute, small, rhythmic. In the cardiac region the heart beat is displaced to the right, which is confirmed by palpation. The heart borders are dilated upwards and to the right, the first sound is clapping, the second sound accent is on the pulmonary artery, there is a presystolic murmur at the apex.
CASE 7
Alan Gray, 67, male, complains of compressing pains in the cardiac area, radiating to the left shoulder, arm, to the region of the 4th-5th finger. The pains are associated with physical exertion and excitement. In addition the patient complains of dyspnea, edema of his feet developing towards night, feeling of heaviness in the right hypochondrium. He has been suffering from pains in the heart area for 10 years, with nitroglycerin relieving them. The pains occurred seldom at first and he was treated as an out-patient. He considers his last setback to be associated with overwork due to an urgent problem at his shop. He works as a senior master at a factory. In the past he had rare colds, smoked much. He drinks alcohol regularly.
Objective findings: he has acrocyanosis, the pulse rate is 106 per minute, rhythmic, of an average fullness, hard. The vascular wall may be palpated outside the pulse wave. The spread heart beat is auscultated in the 5th intercostal space, 2-3 cm from the mediaclavicular line out, on the left. His heart borders are extended to the left, 2 cm from the left mediaclavicular line. The first heart sound is weakened and dull, the second one is accentuated on the aorta. Systolic murmur is heard at the heart apex. Blood pressure is 160 over 70 mm Hg. In the lungs single, moist rales, with somewhat harsh breathing at the background, are heard in the posterobasal parts. The abdomen is soft, tender, the liver edge is palpated 2-3 cm under the ribs, it is round, soft, tender.
DIAGNOSES
The cases above describe:
right pneumothorax associated with an acute attack of chronic bronchitis;
|
|
coronary vascular angina pectoris(stenocardia) with mitral and circulatory insufficiency and cadiosclerosis;
right focal pneumonia of the lower lobe;
lung abcess;
croupous pneumonia;
dry pleurisy associated with pneumonia;
mitral stenosis associated with the left ventricular circulatory failure.
X.Problem Solving
Each of the numbered items in this section is followed by possible answers. Try to select the one lettered answer or completion that is best in each case, discuss it with your partner(s) and comment on your choice trying to prove your decision:
1) An 8-year-old boy with acute lymphoblastic leukemia has had three relapses over the past 2 years. The only available treatment is experimental chemotherapy. Without treatment, the child is unlikely to survive for more than 6 weeks; with treatment his prognosis is unknown. The parents do not want further treatment for their son and wish to take him home; the child also says he wants to go home. Which of the following is the most appropriate course of action?
A) Discharge the child against medical advice;
B) Discharge the child routinely;
C) Petition the court for an order for treatment;
D) Report of the parents to the child protective services for medical neglect.
2) A nurse is hospitalized for appendectomy at the medical center where she is employed. One week after discharge, the assistant hospital administrator asks the surgeon who performed the procedure about the final diagnosis. Which of the following is the most appropriate response on the part of the surgeon?
A) Answer, because it will expedite handling of insurance issues at the medical center;
B) Answer, because as an employee of the medical center the administrator has access to information about patients;
C) Answer, because of the possibility of spreading misinformation about the patient;
D) Decline to answer, because the administrator is not a medical doctor;
E) Decline to answer, because the information is confidential.
3) An asymptomatic 3-year-old boy is brought to the physician for a routine examination. Small, inguinal lymph nodes are palpable; no other abnormalities are noted. Which of the following is the most appropriate next step?
A) Schedule a routine follow-up examination;
B) Urine culture for bacteria;
C) Tape test for pinworms;
D) Monospot test;
E) Complete blood test.
4) A 10-month-old girl, who happily allowed herself to be held when her grandmother visited 2 months ago, now cries when her mother tries to put her in her grandmother’s arms. The most likely explanation is that the child has
A) Been maltreated by the grandmother;
B) Begun to develop problem with socialization;
C) Normal stranger anxiety;
D) A sense of poor relationship between the mother and the grandmother;
E) Separation anxiety disorder.
5) An 8-year-old boy needs to be coaxed to go to school and often, while there, complains of severe headaches or stomach pain. Sometimes his mother has to take him home because of his symptoms. At night, he tries to sleep with his parents. When they insist he sleeps in his room, he says there are monsters in his closet. This history is most consistent with
A) Childhood schizophrenia;
B) Normal concerns of latency-age children;
C) Separation anxiety disorder;
D) Socialized conduct disorder;
E) Symbiotic psychosis.
6) A 70-year-old widower has ecchymosys, perifollicular petechiae, and swelling of the gingival. His diet consists primarily of cola and hot dogs. The most likely diagnosis is
A) Beriberi;
B) Kwashiorkor;
C) Pellagra;
D) Rickets;
E) Scurvy.
7) A 12-year-old girl has incurable muscular dystrophy and has been in a persistent vegetable state for 5 years. Her parents are actually eager to take her to Switzerland to end her life as assisted dying is legal there. Opponents of euthanasia, or ‘mercy killing’, argue that legalization would lead to abuse and call for doctors who participate to be struck off. Those people who are against euthanasia suppose that Public Health Care Service has to organize better palliative care and more hospices for the terminally ill to allow such patients to die with dignity. Which of the following is true to the situation?
A) It’s not correct to continue the critically ill girl’s suffering;
B) You would agree to assist in the death of such a child to end the useless existence;
C) You are against the parents’ position;
D) You are constantly trying to find some experimental drug to help to improve the girl’s condition.
|
|
|
Семя – орган полового размножения и расселения растений: наружи у семян имеется плотный покров – кожура...
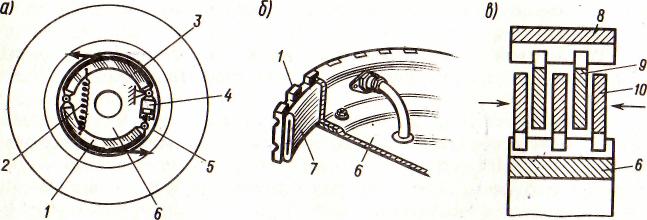
Автоматическое растормаживание колес: Тормозные устройства колес предназначены для уменьшения длины пробега и улучшения маневрирования ВС при...

Типы оградительных сооружений в морском порту: По расположению оградительных сооружений в плане различают волноломы, обе оконечности...
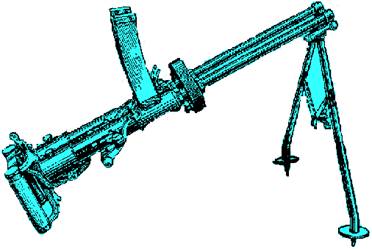
История развития пистолетов-пулеметов: Предпосылкой для возникновения пистолетов-пулеметов послужила давняя тенденция тяготения винтовок...
© cyberpedia.su 2017-2024 - Не является автором материалов. Исключительное право сохранено за автором текста.
Если вы не хотите, чтобы данный материал был у нас на сайте, перейдите по ссылке: Нарушение авторских прав. Мы поможем в написании вашей работы!