
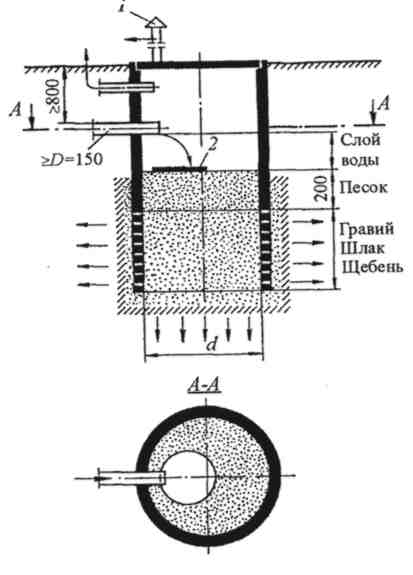
Индивидуальные очистные сооружения: К классу индивидуальных очистных сооружений относят сооружения, пропускная способность которых...
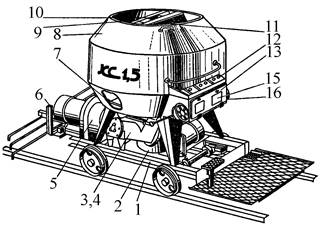
Кормораздатчик мобильный электрифицированный: схема и процесс работы устройства...
Индивидуальные очистные сооружения: К классу индивидуальных очистных сооружений относят сооружения, пропускная способность которых...
Кормораздатчик мобильный электрифицированный: схема и процесс работы устройства...
Топ:
Эволюция кровеносной системы позвоночных животных: Биологическая эволюция – необратимый процесс исторического развития живой природы...
Теоретическая значимость работы: Описание теоретической значимости (ценности) результатов исследования должно присутствовать во введении...
Установка замедленного коксования: Чем выше температура и ниже давление, тем место разрыва углеродной цепи всё больше смещается к её концу и значительно возрастает...
Интересное:
Лечение прогрессирующих форм рака: Одним из наиболее важных достижений экспериментальной химиотерапии опухолей, начатой в 60-х и реализованной в 70-х годах, является...
Принципы управления денежными потоками: одним из методов контроля за состоянием денежной наличности является...
Наиболее распространенные виды рака: Раковая опухоль — это самостоятельное новообразование, которое может возникнуть и от повышенного давления...
Дисциплины:
|
из
5.00
|
Заказать работу |
|
|
|
|
1. Какой нерв иннервирует и осуществляет секреторную функцию подчелюстной и подъязычной желез?
1. Промежуточный.
2. Верхнечелюстной.
3. Подъязычный
2. Какие нервные волокна в системе лицевого и промежуточного нервов осуществляют иннервацию подчелюстной и подъязычной слюнных желез?
1. Большой каменистый нерв.
2. Барабанная струна.
3. Стременной нерв.
3. С какими черепными нервами промежуточный нерв имеет общее вкусовое ядро одиночного пути?
1. С языкоглоточным.
2. С блуждающим.
3. С тройничным.
4. У больного внезапно развилась следующая неврологическая симптоматика в правой половине лица: больной не может поднять бровь, зажмурить глаз, надуть щеку, открыть рот в полном объеме, имеется слезотечение справа. Функция какого нерва нарушена?
1. Тройничного.
2. Лицевого.
3. Глазодвигательного.
5. Определить уровень поражения лицевого нерва, если у больного выявляется слева сухость глаза, симптом Белла, сглаженность носогубной складки, нарушение вкуса на передних 2/3 языка, лагофтальм, гиперакузия.
1. Область околоушной слюнной железы.
2. Внутренняя капсула.
3. Ствол мозга.
4. Канал лицевого нерва.
6. Больной оперирован в стоматологическом отделении по поводу кисты околоушной слюнной железы справа, после чего у пациента возникли следующие симптомы: не может собрать в складку лобную мышцу, имеется редкое мигание, слезотечение из правого глаза, веки не смыкаются, сглажена правая носогубная складка, симптом «ракетки» справа. Какой нерв пострадал вследствие хирургического вмешательства?
1. Нижнеглазничный.
2. Лицевой.
3. Глазодвигательный.
7. Больной утром после сна заметил припухлость губ, слизистой рта. Через несколько часов «перекосило лицо», появилась болезненность и затруднение движения языка. При обследовании выявлено: отек губ, языка, периферический парез лицевого нерва. Определить синдром?
|
|
1. Синдром Сладера.
2. Синдром Шегрена.
3. Синдром Мелькерсона—Розенталя.
8. Какой симптом не характерен для синдрома Мелькерсона—Розенталя?
1. Парез лицевого нерва по периферическому типу.
2. Гранулематозный глоссит.
3. Отек губ.
4. Герпетические высыпания в области щек и верхней губы.
9. Какие структуры заинтересованы при синдроме Мелькерсона—Розенталя?
1. Кора головного мозга.
2. Гипоталамус.
3. Ствол мозга.
10. Больному под местной анестезией (ультракаин 2 мл) удален зуб. Спустя 15 минут у него развился отек Квинке. Для оказания помощи какой препарат ему не нужно было вводить?
1. Преднизолон.
2. Супрастин.
3. Пенициллин.
4. Кордиамин.
11. У больного увеличены слюнные железы, сухость слизистых оболочек, затруднение жевания и глотания. Определить синдром.
1. Синдром Сладера.
2. Синдром Шегрена.
3. Синдром Ханта.
12. Какой симптом не характерен для синдрома Шегрена?
1. Паротит.
2. Кератоконъюнктивит.
3. Парез мимических мышц.
13. У больного резкие приступообразные боли и герпетические высыпания в области правой ушной раковины и наружного слухового прохода, нарушение вкуса и гиперстезия в области передних 2/3 языка, парез мимических мышц на правой половине лица. Определить синдром.
1. Синдром Сладера.
2. Синдром Мелькерсона—Розенталя.
3. Синдром Ханта.
14. Определить какой симптом будет постоянным при невралгии узла коленца, синдроме Ханта?
1. Периферический парез лицевого нерва.
2. Герпетические высыпания в области ушной раковины.
3. Снижение слуха.
15. У больного приступы болей в области корня языка, распространяющиеся на мягкое небо, горло, ухо. Приступы провоцируются движениями языка, приемом горячей пищи, слюна на стороне боли более вязкая. При пальпации болезненность в области угла нижней челюсти на одноименной стороне. Определить синдром.
|
|
1. Невралгия нижнечелюстного нерва.
2. Невралгия языкоглоточного нерва.
3. Невралгия верхнегортанного нерва.
16. После операции по поводу кисты дна полости рта у больного возникли боли в корне языка, язык отклоняется в сторону поражения и имеется незначительная атрофия мышц языка на стороне поражения. Какой нерв пострадал вследствие хирургического вмешательства?
1. Язычный.
2. Подъязычный.
3. Языкоглоточный.
17. У больного приступообразные боли в области глазного яблока. Во время приступа отмечается покраснение конъюнктивы глаза, слезотечение, светобоязнь, обильное выделение носового секрета. Определить синдром.
1. Невралгия носоресничного нерва (синдром Чарлина).
2. Поражение ресничного узла (синдром Оппенгейма).
3. Невралгия узла коленца (синдром Ханта).
18. Больной обратился к врачу с жалобами на боли в правом глазном яблоке, слезотечение, покраснение глаза. В области кожи лба герпетические высыпания. Глазное яблоко при пальпации болезненно. Определить синдром.
1. Синдром Оппенгейма, поражение ресничного узла.
2. Синдром Чарлина, невралгия носоресничного нерва.
3. Синдром Сладера, поражение крылонебного узла.
19. Больного беспокоят приступообразные боли в височной области слева, кпереди от наружного слухового прохода, боль иррадиирует в нижнюю челюсть, зубы, шею. Определить синдром.
1. Синдром крылонебного узла.
2. Невралгия первой ветви тройничного невра
3. Невралгия ушно-височного нерва.
20. У больного отмечаются боли в области виска, внутри уха, передней стенки наружного слухового прохода, в области височно-нижнечелюстного сустава. В околоушной области — покраснение кожи и капельки пота. Усиленное слюноотделение. Определить синдром.
1. Невралгия ушно-височного нерва.
2. Поражение ушного узла.
3. Невралгия носоресничного нерва (синдром Чарлина).
21. Какой нерв не входит в систему I ветви V нерва?
1. Лобный.
2. Слезный.
3. Подглазничный.
4. Носоресничный.
22. Какой нерв не относится к концевым ветвям 2-й ветви тройничного нерва?
1. Скуловой.
2. Ушно-височный.
3. Подглазничный.
4. Носоресничный.
23. Какой нерв не относится к концевым ветвям 3-й ветви тройничного нерва?
1. Язычный.
2. Щечный.
3. Нижний альвеолярный.
4. Крылонебные ветви.
24. Какой вегетативный узел относится к 1-й ветви тройничного нерва?
|
|
1. Крылонебный.
2. Околоушный.
3. Ресничный.
4. Подчелюстной.
25. Какой вегетативный узел относится к 2-й ветви тройничного нерва?
1. Ресничный.
2. Крылонебный.
3. Околоушный.
4. Подъязычный.
26. Какой вегетативный узел не относится к 3-й ветви тройничного нерва?
1. Подчелюстной.
2. Подъязычный.
3. Крылонебный.
4. Околоушный.
27. Для лечения невралгии тройничного нерва приступа какой препарат следует выбрать?
1. Анальгин.
2. Карбамазепин.
3. Витамин В12.
4. Сульфадемитоксин.
28. Какой препарат следует выбрать для купирования одонтогенной боли?
1. Карбамазепин.
2. Анальгин.
3. Витамин В12.
4. Сульфадемитоксин.
29. Ночные боли в челюстно-лицевой области характерны:
1. Для невралгии тройничного нерва.
2. Для острого пульпита.
3. Для среднего кариеса.
30. Через какое образование ветви V нерва не выходят на лицо?
1. Надглазничная вырезка.
2. Шило-сосцевидное отверстие.
3. Подглазничное отверстие.
4. Подбородочное отверстие.
Перечень итоговых вопросов:
1. Исследование функции I-VI черепных нервов.
2. Системная организация речевой функции, виды расстройства речи.
3. Понятие о начальных проявлениях недостаточности кровоснабжения мозга.
4. Исследование функции VII-ХII пар черепных нервов.
5. Понятие о функциональной асимметрии больших полушарий мозга.
6. Атеросклероз сосудов головного мозга, дисциркуляторная энцефалопатия.
7. Исследование сухожильных и кожных патологических рефлексов.
8. Системная организация произвольных движений. Роль пирамидной системы, симптомы поражения.
9. Субарахноидальное кровоизлияние. Геморрагический инсульт.
10. Исследование вегетативной нервной системы.
11Синдромы поражения лобной доли головного мозга.
12.Преходящие нарушения мозгового кровообращения.
13.Исследование менингеальных симптомов.
14.Синдромы поражения затылочной доли.
15.Ишемический инсульт.
16.Исследование болевых точек и симптомов натяжения нервных стволов.
17.Синдром поражения теменной доли головного мозга.
18Неотложная помощь при нарушении мозгового кровообращения. Базисная и дифференциальная терапия.
19.Неотложная помощь при нарушении мозгового кровообращения. Базисная и дифференциальная терапия.
|
|
20.Синдромы поражения височной доли головного мозга.
21.Абсцесс головного мозга.
22.Ультразвуковые методы исследования.
23.Синдромы поражения внутренней капсулы.
24.Вторичный гнойный менингит. Дифференциальная диагностика с менингококковым менингитом.
25.Понятие об электрофизиологических методах исследования нервной системы.
26.Гипоталамический синдром.
27.Вторичные серозные менингиты. Туберкулезный менингит.
28.Исследование функции I-VI черепных нервов.
29.Синдром поражения ножки мозга.
30.Классификация нейростоматологических заболеваний.
31.Исследование функции VII-ХII пар черепных нервов.
32.Синдром поражения продолговатого мозга.
33.Невропатии лицевого нерва. Компрессионно-ишемические невропатии.
34.Исследование поверхностной и глубокой чувствительности.
35.Синдром бульбарного и псевдобульбарного паралича.
36.Дентальная плексалгия
37.Методы исследования XII пары черепных нервов.
38.Вегетативная нервная система.
39.Закрытая черепномозговая травма. Ушиб головного мозга.
40.Исследование функции лицевого нерва.
41.Надсегментарный уровень вегетативной нервной системы.
42.Неврологические осложнения остеохондроза позвоночника.
43.Исследование функции тройничного нерва.
44.Спастический паралич.
45.Принципы диагностики и неотложной терапии внутричерепных гематом.
46.Исследование функции IX пары черепных нервов.
47.Вялый паралич.
48.Сотрясение головного мозга (клиника, диагностика, лечение).
49.Исследование функции X пары черепных нервов.
50.Вегетативная иннервация лица.
51.Одонтогенные менингиты.
52.Исследование функции VII пары черепных нервов.
53.Бульбарный синдром.
54.Сочетанные черепномозговые и лицевые травмы.
55.Исследование V пары черепных нервов.
56.Вегеталгии.
57.Невралгии языкоглоточного нерва.
58.Исследование менингеальных симптомов.
59.Прозопарезы.
60.Невралгия тройничного нерва.
II.Материалы, устанавливающие содержание и порядок проведения промежуточных и итоговых аттестаций –
VIII семестр – зачет.
Дополнительно для ФОИС –
3.5. Методические указания студентов
LESSON 1. MOVEMENT SYSTEM.
QUESTIONS
1) How many neurons are included into the corticospinal tract?
2) What is the other name of the corticospinal tract?
3) Why is the corticospinal tract called as the pyramidal?
(2 variants).
4) Where is a cortex centre of the movement system located?
5) What anatomical features are there in the cortex exposition of the body and limbs in the precentral gyres?
6) Describe the anatomical way of the upper motoneuron.
7) Describe the pathways of the lower motoneuron.
8) Where is a crossing of both corticospinal tracts located?
9) Which structures of the lower motoneuron lead the nerve roots to the segments of the spinal cord?
10) Which structures of the lower motoneuron lead the nerve roots to the limbs and body?
11) Which segments of the spinal cord lead the nerve roots to the muscles of the head and neck? Which segments of the spinal cord lead the nerve roots to the muscles of the shoulder girdle and upper extremities?
|
|
12) Which segments of the spinal cord lead the nerve roots to the muscles of the body?
13) Which segments of the spinal cord lead the nerve roots to the muscles of the pelvis girdle and lower extremities?
14) Where is the centre of an autonomic innervation’s of a bladder and bowel located?
15) Which pathological sings are positive?
16) Which pathological sings are negative?
17) What complex of signs and symptoms include a clinical picture of the upper motoneuron paralysis?
18) What complex of signs and symptoms include a clinical picture of the lower motoneuron paralysis?
19) Describe the precentral gyres syndrome.
20) What signs of damage are present in subcortical structures? Describe the difference between the damage of corona radiate and internal capsule of the damage of the brainstem.
21) Describe the characteristic signs of disturbances on the level C1-C4.
22) Describe the characteristic signs of disturbances on the level C5-C8.
23) Describe the characteristic signs of disturbances on the level Th1-Th12.
24) Describe the characteristic signs of disturbances on the level L1-L4.
25) Describe the characteristic signs of disturbances on the level L5-S2.
26) What are the types of epileptic seizures, which are present in precentral gyres syndrome? What kinds of seizures develop in this syndrome?
27) Describe the epicones syndrome.
28) Describe the cones syndrome.
29) What is the difference between central and peripheral types of the bladder and bowel dysfunctions?
Task 1.
Two hours prior to admission to the emergency ward a 52 year- old man developed right arm, hand and leg weakness. At the time of examination, dysphasia and right face drooping were noted. Over the ensuing hour the patient became obtunded, areflexic on the right side, and completely unable to lift the right arm against gravity. The physical exam added no new information.
● What syndrome is revealed in the patient?
● What structures are involved?
● Where is the focus of the lesion?
Task 2.
A 65 year-old man complained of weakness in the right arm. For 3 months he had been dropping objects, and it was gradually getting worse. There were no sensory symptoms. On exam, the patient was mildly confused and speech was slow and slurred. The right nasolabial fold was flat. Muscle bulk was normal. No fasciculations were seen. Rapid passive movements of the right arm or leg met with resistance which would give way ("clasp-knife"). Strength was minimally diminished in the right intrinsic hand muscles, the wrist dorsiflexors, triceps, deltoids, iliopsoas, hamstrings and tibialis anterior. A right pronator drift was observed. Finger movements were slow on the right. The right leg circumducted while walking. Reflexes were hyperactive on the right. The right plantar response was extensor. Sensation to touch, pin, cool, vibration was normal. Two-point discrimination, point localization and graphesthesia were poorly done on the right in comparison with the left.
● List features of the clinical upper motoneuron and low motoneuron syndrome.
● What are possible sites of weakness in this case?
● Give a few etiological possibilities.
Task 2.
А 62 year old man complains of tremor of the right hand for six months. It began with an occasional tremor of the right thumb but has gradually spread to all fingers and is now continuous. He has also noticed that his handwriting has become smaller and more difficult to read. It is harder for him to use a toothbrush with the right hand and his wife must help him button the left shirt sleeve. She has observed that her husband occasionally drools and that his voice is softer. On examination, the patient is mentally normal but often responds slowly. The voice is soft and monotone. Facial expression and blink rate are diminished. He pushes off with his hands when arising from a chair and the gait is slowed with short steps and decreased arm swing on the right. There is a slow, resting tremor of the right hand which suppresses with maintenance of a posture. There is an occasional, asymptomatic tremor of the right foot. There is cogwheel rigidity in both upper extremities, the right more than left, with slowed repetitive movements of the right hand and foot.
-What is the diagnosis?
-Distinguish the following tremors: Parkinson's, Essential, Cerebellar.
-What is meant by "tone?" Distinguish flaccidity, spasticity, cogwheel rigidity, and paratonic ("lead-pipe") rigidity.
-What are the classical symptoms and signs of Parkinson's Disease?
Task 3.
You are asked to consult on a 35 year old woman hospitalized on the psychiatry service for evaluation of "muscle twitches." The patient is currently hospitalized for depression and anxiety. Further history reveals that the patient's work performance has declined over the past year associated with changes in personality and occasional poor judgment. The patient's family history reveals that her father died at age 50 in a nursing home of "Alzheimer's disease." The patient's paternal grandmother died in a mental institution of unclear cause. The patient's brother is described as being "restless." The patient's children are healthy. On examination, the patient is dysarthric and shows impaired memory and concentration on mental status testing. She has irregular "jerky movements," of the hands, feet, and trunk. These are rapid and non-stereotyped. The patient's saccades are slow but with full eye movements. There is a milkmaid's grip. The patient has an unusual gait disorder, placing the feet irregularly with a tendency to trip and demonstrate
"dancing like" movements.
● What type of hyperkinesia is in the patient?
● What is chorea? Be able to differentiate it from tremor, myoclonus, and dystonia.
● What neuroimaging finding is seen in Huntington's disease?
Lesson 2: Sensory system
QUESTIONS
22. What view does the area of presentation of hypo- or anesthesia in neural type of sensations disorder have?
23. What view does the area of presentation of hypo- or anesthesia in polyneural type of sensations disorder have?
24. What view does the area of presentation of hypo- or anesthesia in spinal conductive type of sensations disorder have?
25. What view does the area of presentation of hypo- or anesthesia in segmental spinal type of sensations disorder have?
Task 1.
A 55 year old right-handed man presented with a 4 hour history of weakness and tingling of his right hand and numbness of the right side of his mouth. Mild difficulty was experienced with word finding. Symptoms had improved since onset, but had not fully resolved. There was no significant past symptomatology.
Vital signs and general physical exam were normal. Mental status and speech were normal. Right nasolabial fold was flat relative to the left, but all other cranial nerve functions were intact. Subjective numbness was noted over the right distal hand, with errors exhibited in tests for two-point discrimination and graphesthesia. A mild right arm pronator drift and clumsiness of finger tapping in the right hand were observed. Reflexes were slightly more active on the right. The right toe was upgoing.
● What syndromes are revealed in the patient?
● Where is the likely focus of the lesion?
Task 2.
А 47 year-old right-handed man developed progressive numbness of both feet over a 6 month period. Recently, his fingertips started feeling numb. He described an unpleasant burning sensation. Weakness was denied.
On exam, mentation and cranial nerves were normal. There were no palpably enlarged nerves, nor high arches. Position and vibration sense were grossly diminished in the feet. Cool stimuli and pin were perceived, but there was a subjective stocking distribution of numbness to mid-calf bilaterally. Reflexes were absent at the ankles and diminished elsewhere. Strength was close to normal, except that he could not walk on his heels.
● What type of sensory disorder is there?
● Is there evidence for autonomic involvement? What points in the history and exam might be explored to test this?
Lesson 3: Cranial nerves
Questions
Task 1.
A 50 year-old woman complained of dizziness when she moved her head when turning over in bed. She was otherwise well and without antecedent illness or medical history of note. Exam demonstrated transient torsional-vertical nystagmus after the patient quickly moved her head back with the right ear down.
● Give a general approach to the "dizzy patient". Begin with likely causes of dizziness.
● When is dizziness "vertigo". What are some important etiologies of vertigo?
● What studies can be done to clarify the etiology of vertigo?
● What is the most likely diagnosis in this case? How would you advise and treat the patient?
Task 2.
A 33 year-old woman slowly developed tinnitus and lost hearing in her left ear over a 2 year period. There were no other reported symptoms. Exam confirmed decreased acuity on the left, with air conduction greater than bone conduction bilaterally, and Weber lateralizing to the right ear. The left corneal reflex was diminished. A mild clumsiness and intention tremor was noted in the left hand.
● What is the differential diagnosis of hearing loss in one ear?
● What neural systems are impaired in this woman? What is the likely diagnosis?
Task 3.
A 63 year-old man presented to the emergency room because he was unable to see objects to his left. This came to his attention when he was sideswiped by a garbage truck in cross-traffic. On examination he had a left homonymous hemianopsia. Saccades could be made in all directions but smooth eye movements were interrupted by frequent saccadic eye movements. The remaining neurological exam was negative.
● What is the course of fibers from retina to occipital lobe?
● What is the significance of:
Homonymous hemianopia?
Heteronymous hemianopia?
3. Homonymous superior quadrantinopia?
● What is the significance of congruity in a field defect?
● What is the significance of the smooth pursuit defect in this case?
Task 4.
A 25 year-old R.N. suddenly notices that her left pupil is larger than her right (5 vs 3 mm).
● What is the pathway mediating the pupillary light reflex?
● What is the differential diagnosis of anisocoria?
● What is a "IIIrd nerve palsy"? A "Homer's Syndrome"? What do each signify?
|
|
|
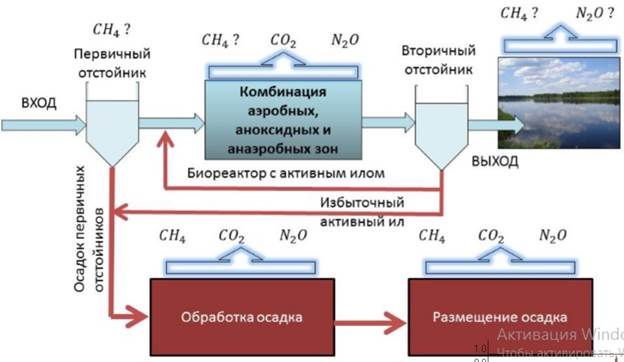
Эмиссия газов от очистных сооружений канализации: В последние годы внимание мирового сообщества сосредоточено на экологических проблемах...
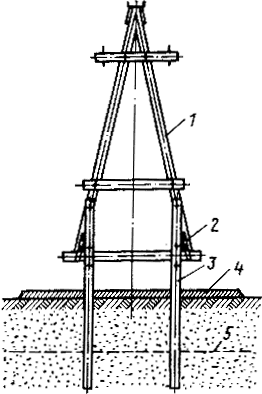
Особенности сооружения опор в сложных условиях: Сооружение ВЛ в районах с суровыми климатическими и тяжелыми геологическими условиями...

Таксономические единицы (категории) растений: Каждая система классификации состоит из определённых соподчиненных друг другу...
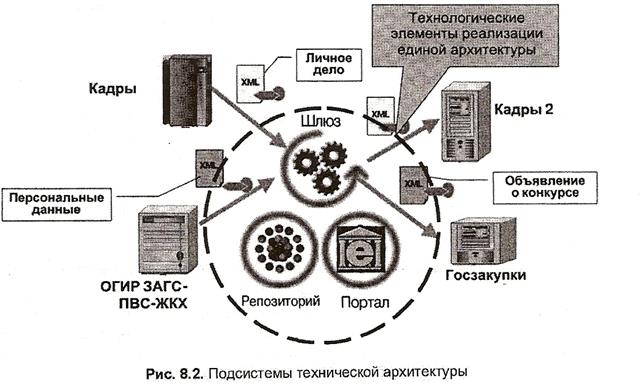
Архитектура электронного правительства: Единая архитектура – это методологический подход при создании системы управления государства, который строится...
© cyberpedia.su 2017-2024 - Не является автором материалов. Исключительное право сохранено за автором текста.
Если вы не хотите, чтобы данный материал был у нас на сайте, перейдите по ссылке: Нарушение авторских прав. Мы поможем в написании вашей работы!